Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Bodyfocushealthgroup.com.au
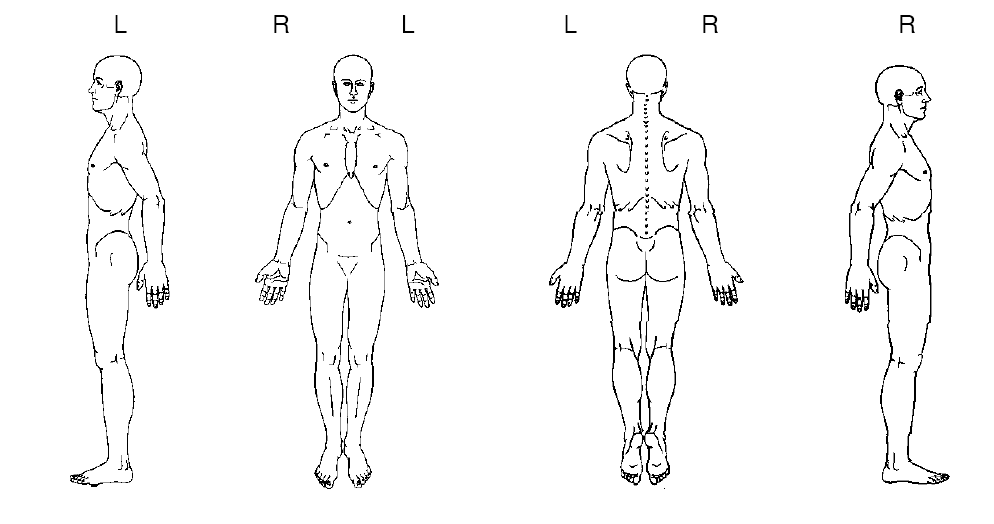
CONFIDENTIAL PATIENT CASE HISTORY As a multidisciplinary practice providing comprehensive care, we focus on your ability to be healthy. Our goals are: firstly, to address the issues that brought you to this practice; secondly, to treat the cause of your condition (not just treat the symptoms or place a temporary patch over your condition); and thirdly, to offer you the opportunity of improved health potential and wellness services in the future. Answering the following questions will give us a profile of your health, and ensure that we optimise your outcome and deliver treatment excellence. What is your major complaint? _________________________________________________________________ Draw on the sketch below the area(s) where you feel your problem to be.
When did your symptoms start? _________________________________________________________________ Was it a gradual or sudden onset? _________________________________________________________________ Have you had this or a similar problem in the past? _________________________________________________________________ If you are experiencing pain, please tick the words that best describe your pain:
Confidential Patient Case History Form Version 1.0,
Do you get?
needles Since the problem started it is:
About the same Getting better Getting worse
What makes your pain worse? Your pain interferes with: What type of work do you do? __________________________________________________________ Any Bladder or Bowel changes since this episode started? __________________________________________________________ Do you experience any nausea, dizziness, difficulty swallowing, changes in vision, or fainting spells, fever, skin rashes associated with your symptoms? __________________________________________________________ Other health professionals seen for this problem (please list): Medical Doctor____________________________________________________________ Specialist Doctor/Surgeon_____________________________________________________ Physiotherapist/Chiropractor __________________________________________________________________ Other __________________________________________________________________ List any medications you are taking __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ Have you ever taken oral cortisone or prednisone (including asthma medications such as pulmicort, symbicort, flixotide & seretide)? Y/N Are you pregnant? Y/N
Confidential Patient Case History Form Version 1.0,
Do you have or have you ever had?: (please tick)
High blood pressure
Patient’s Signature: _______________ Print Name: ______________________ Practitioner's Signature: _________________ Date: _____________________
Confidential Patient Case History Form Version 1.0,
Responsabile del Centro Emostasi e TrombosiSIMG,Società Italiana di Medicina Generaleper la Sorveglianza degli Anticoagulati (FCSA)SIMG,Società Italiana di Medicina GeneraleLa realizzazione e distribuzione di questo fascicolo è stata resa pos-sibile grazie al contributo di Ravizza Farmaceutici SpA PREFAZIONE La terapia anticoagulante orale (TAO) costituisce un tratta-mento di grande e cr
CONVOCATORIA Y DATOS GENER ALES DEL PROCE SO DE CONTRATACI ÓN S ERVICIO MUNIC IP AL DE AGUA P OTABLE Y AL CANT ARILLADO SANIT ARIO DE C OCHABAMBA - SEMAPA 1. CONV OCATOR IA Se convoca a la p resen tación de p ropuestas para el sig uiente proceso : S ERV ICIO MUNIC IPA L DE AGU A PO TAB LE Y AL CAN TAR ILLA DO S ANIT ARI O DE En tidad Convocan te : CO CHA BAMB A Mo d

 CONFIDENTIAL PATIENT CASE HISTORY
CONFIDENTIAL PATIENT CASE HISTORY 
 Do you have or have you ever had?: (please tick)
Do you have or have you ever had?: (please tick)