Journal of Orthodontics, Vol. 34, 2007, 6–11
M. A. Hain, L. P. Longman, E. A. Field, J. E. HarrisonLiverpool University Dental Hospital, Liverpool, UK
Natural rubber latex (NRL) allergy can have potentially serious consequences, and reports of orthodontic patients reacting toNRL have increased significantly over recent years. It is therefore important for the orthodontist to know how to managepatients with an NRL allergy and how to deal with possible reactions to NRL. Safe and effective practice depends onrecognizing patients who are at risk of NRL allergy, and an awareness of materials and equipment that contain NRL and theavailability of suitable NRL-free alternatives.
Key words: NRL, elastics, rubber, latex, allergy, latex-free
Received 20th February 2006; accepted 29th April 2006
NRL gloves,1,5 and a third related the development ofstomatitis to the use of orthodontic elastics.6 Jacobsen
Exposure to natural rubber latex (NRL) in the clinical
and Pettersen surveyed Norwegian orthodontists who
environment has increased significantly since the mid-
had treated approximately 41,000 patients from 1998 to
1980s because of concerns over the transmission of viral
2000. This group reported 14 reactions to elastics and
infections, such as human immunodeficiency virus (HIV)
one anaphylactoid reaction to gloves. The commonest
and hepatitis B. This has resulted in protective gloves,
sites affected were the gingivae and tongue, but the
usually made from NRL, being worn routinely for
perioral region was also affected. The data were
clinical procedures where contact with bodily fluids may
collected by questionnaire, and an ‘assumed’ causal link
occur. The increase in the use of NRL clinical gloves has
been accompanied by a rise in the incidence of NRL
NRL sensitivity is associated with atopy, reflecting a
allergy in health-care workers (HCWs) and patients.1,2
predisposition to producing IgE antibodies. The main
This article describes possible reactions to NRL in
types of reaction to NRL are irritant contact dermatitis,
orthodontics. After a brief description of the processes
allergic contact dermatitis and NRL allergy. Owing to
underlying the different reactions to NRL, the diag-
the uncertainties regarding the diagnostic reliability of
nosis and orthodontic management considerations are
the current tests, estimates of the prevalence of NRL
allergy vary considerably, depending on which diagnos-
Jacobsen and Hensten-Pettersen found that, from
tic tests are used and the population tested. The
1998 to 2000, there had been a ten-fold increase in
prevalence of NRL allergy has been reported as being
reported reactions to NRL during orthodontic treat-
less than 1% in the general population, 5–15% in HCWs
ment, while reports of reactions to the metallic
and 24–60% in patients with spina bifida.7
components used during orthodontic treatment had
A standard medical history should identify patients
actually decreased.1 In orthodontics, as well as in the
with confirmed NRL allergy. However, additional
gloves that are routinely worn when treating patients,
information pertinent to NRL allergy should be sought
NRL is also present in other materials such as inter- and
to help identify other patients at potentially increased
intra-arch elastics. These elastics often play an impor-
risk of developing NRL allergy. Hypersensitivity to
tant part in orthodontic mechanics, due to their ability
certain foods such as avocados, potatoes, bananas,
to exert a predictable force and their low cost.3 Other
tomatoes, chestnuts, kiwi fruit and papaya is associated
sources of NRL are discussed later in the article.
with NRL allergy.8 A history of ‘asthma-like’ symptoms
Russell et al. found only three reports in the literature
relating NRL allergy to orthodontic treatment.4 Two of
exposure to NRL-containing products also requires
these studies related the allergic reaction to the use of
Address for correspondence: Max Hain, Orthodontic Department,Liverpool University Dental Hospital, Pembroke Place, L3 5PS, UK. Email: [email protected]# 2007 British Orthodontic Society
patient may also complain of a burning or itchingsensation in the affected area.11,12 Allergic contact
An awareness of how NRL is manufactured and an
dermatitis is not a life-threatening condition, and there
appreciation of the processes underlying the different
is no firm evidence of any immunological association
reactions to NRL-containing materials are helpful when
between Type I NRL allergy and the Type IV reaction
trying to understand and manage the clinical issues.
NRL is the sap of the commercial rubber tree Havea
A patient who gives a history of a reaction to NRL
brasiliensis and contains over 200 polypeptides, not all
elastics that resolves upon changing the brand of
of which are recognized as allergens. NRL is used either
elastics12 is likely to have had a Type IV reaction to a
to produce dry rubber goods, such as tyres, or dipped
chemical present in one brand of NRL elastics and not
goods, such as gloves. During the manufacturing pro-
in the other. It may be possible to distinguish allergic
cess, various chemicals, e.g. thiurams and carbamates,
contact dermatitis from irritant dermatitis by noting the
are added to the NRL. These additives have long been
extent of the spread of the reaction. Allergic contact
recognized as a cause of allergic contact dermatitis.7
dermatitis can often spread beyond the area of physicalcontact;13 however, in most cases it will be the history
and clinical presentation, followed by patch testing, thatwill confirm the diagnosis.
The diagnosis of NRL contact allergy is advantageous
from both the patient and HCW perspective. The
Irritant contact dermatitis is the most frequent cause of
management of patients with delayed Type IV allergic
hand eczema. It results from a combination of chemical/
contact dermatitis is less problematic than the manage-
mechanical irritation and is not an allergy to proteins or
ment of patients with NRL allergy. Although the history
can be quite effective at identifying this latter group of
Typically, irritant contact dermatitis starts along skin
patients, it is essential that an appropriate specialist
folds or under a ring and tends to present as dry irritable
makes the diagnosis. While allergic contact dermatitis is
patches or as chapping on the hands. Predisposing
not a life-threatening condition, it is still desirable to
factors include perspiration trapped under gloves and
minimize NRL exposure for this group of patients.
residue from soaps. The use of an appropriate hand
NRL-free gloves and materials should therefore be used
protection regime will minimize the risk of developing
(Table 1). It is, however, not essential to treat patients
hand dermatitis. It has been suggested that eczematous
with an NRL contact allergy in a ‘latex-screened’
skin is less of a barrier to allergens, so that subsequent
sensitization may be more likely. Members of the dentalteam who develop any of the above signs or symptoms
should have patch testing carried out to exclude allergiccontact dermatitis.
NRL allergy results from an immediate (Type I) IgEantibody-mediated response to NRL and usually occurs
within 5–60 minutes of contact with NRL. However, thethresholds for sensitization and reaction are unknown.7
Allergic contact dermatitis is the result of delayed
Severe systemic reactions, involving the skin, airways
hypersensitivity (Type IV), and is a cell-mediated
and/or cardiovascular systems, have been reported after
response to specific chemicals referred to as contact
cutaneous and respiratory exposure. Mucosal and
sensitizers. The allergens usually responsible for trigger-
parenteral exposure to NRL allergens pose the greatest
ing the allergic reaction are the chemical accelerators
risk of anaphylaxis.7 Powder has traditionally been
(thiurams, carbamates and benzothiazoles) that are used
added to gloves to facilitate donning. The powder
in the glove-manufacturing process. At present, it is not
(usually corn starch) has been shown to adsorb NRL
clear whether NRL proteins may themselves cause a
proteins and therefore acts as a vehicle for the
Allergic contact dermatitis can result in an eczematous
Aeroallergens have the potential to be potent sensitizers.
rash that is typically pruritic. The skin may also be scaly,
The discontinuation of the use of powdered NRL gloves
swollen or vesicular and weeping, with any reaction
appeared to have been effective at reducing sensitization
tending to peak approximately 48 hours after exposure
of dental students to NRL in one study.14
to the allergen. If the mucosa is involved, it may swell,
The face, especially the lips and mouth, is likely to be
become erythematous or develop small vesicles. The
affected first if a dental patient develops an acute allergic
reaction to NRL. The patient’s skin usually becomes
In the light of current information, it seems prudent
itchy and develops weals, giving the skin a ‘nettle rash’
that when treating patients with clinical and immuno-
appearance. This may resolve in a relatively short
logical evidence of NRL allergy, contact with potential
allergens should be avoided.7,8,16 Members of the dental
reaction may progress to involve the patient’s airways
team therefore need to be familiar with and strictly
and/or develop into a full anaphylactic reaction. If
adhere to NRL avoidance protocols in order to protect
untreated, anaphylaxis may lead to a cardiac arrest.
patients or staff with an NRL allergy. It may be that asknowledge and diagnostic techniques improve, these
precautions will be shown to be over-zealous.16
Patients suspected of having an NRL allergy should bereferred to an appropriate expert (usually an allergist,
clinical immunologist or dermatologist) for testing. At
present, none of the available tests for NRL allergy
The remaining sections of this article relate specifically
demonstrates complete diagnostic reliability. Despite
this, it is usually possible to confirm a suspecteddiagnosis of a Type I NRL allergy by skin prick testing
Patients with suspected or proven NRL allergy
or immunoassay to detect NRL-specific IgE antibodies. However, Cullinan et al. stated that agreement between
the results of skin prick testing and serological assays is
Exposure of patients who are sensitized to NRL to a
product containing NRL could be potentially fatal. It is
Skin prick testing involves placing NRL extract
diluted in saline on the skin and scratching the skinwith a needle. The reaction is then compared to that
N manage the patient in a ‘latex-screened’ environment;
obtained with a histamine control.15 Immunoassays
N monitor the patient for signs of adverse reactions;
such as radio-allergosorbent testing (RAST) measure
N ensure that resuscitation equipment is free from
NRL-specific IgE to various allergy extracts. The
patient’s serum is initially reacted with the allergen
N ensure the capability of NRL-free delivery of emer-
and then incubated with radiolabelled anti-human
IgE.15 The presence of positive IgE test results, in theabsence of clinical symptoms of NRL allergy, suggests
Creation of a ‘latex-screened’ dental environment
cross-reactivity to other allergens. Structural homolo-gies between Havea proteins and other plant/fruit
It is not feasible to achieve the total elimination of NRL
from the dental environment (for example, staff clothes
Examples of NRL-free products for use in orthodontics.
GAC (www.gacintl.com): NRL-Free Elastics; Leone (www.leone.it); Dentaurum ([email protected]):intra-oral elastics
3M Unitek (3M.com): Alastic range of power chain and modules; Dentaurum Dentalastics: plasticligatures, ligature chain, rotation wedges, ‘Personal’ coloured modules, Elasto-Force plastic chain; TPOrthodontics ([email protected]): ligatures, e-links, e-chain
TP Orthodontics: headgear components; 3M Unitek: headgear components, except lining in chin cupwhich does contain NRL
TP Orthodontics: self-locking separator springs, sep-a-rings; Dentaurum Dentalastics: separators
Damon (www.ormco.com); Speed (www.speedsystem.com); Innovation (GAC); SmartClip (3M Unitek)
Contra petite Web disposable (www.youngdental.com)
Kimberly-Clark (www.kchealthcare.com): Safeskin Purple Nitrile; Bodyguards Nitrile Gloves(www.medisavers.co.uk); Schottlander (www.schottlander.co.uk): NRL-Free Nitrile; Regent(www.regentmedical.com): Biogel Skinsense PI
Kimberly-Clark: Technocol Soft, Technocol Fluidshield
This table is not exhaustive, and manufacturing processes may change. It is prudent to check with the manufacturer that their products are NRL free.
may contain NRL elastic). The aim is therefore to create
showed greater force decay, and it was concluded that
a ‘latex-screened’ environment in which exposure to
great improvements in the physical properties of the
NRL is reduced as far as is reasonably possible. NRL
silicone bands would be required before they could be
exposure can be minimized by measures such as
considered as an acceptable alternative to NRL elastics.
decontamination of the surgery with a ‘protein wash’
After static force extension of 450% for 1 day in saliva,
and storing the NRL-free products in a ‘latex-screened
the force decay was 33% for the silicone bands and 28%
surgery’ to avoid prior contamination by storage with
for the NRL elastics.17 Russell reported that NRL-free
NRL materials. NRL-free gloves must be worn in the
elastics showed greater hysteresis than NRL elastics
latex-screened facility, and powdered NRL gloves
(40% force decay as opposed to 25% over 24 hours;
should never be available in a clinical environment.
furthermore, the range of forces produced by the NRL-
Whether an orthodontic practice can be designated as
‘NRL-screened’ depends on a number of factors,
The ideal force required to maximize the rate of tooth
including: staff experience and training, especially in
movement is still unknown, although most evidence
the management of medical emergencies; the availability
would suggest that there is a wide force spectrum to
of NRL-free drugs and equipment; the organization of
which teeth will respond appropriately.18 Clinical trials
the practice; and financial and time constraints.16 It is
comparing rates of tooth movement in response to
helpful to divide the clinical management of patients
mechanics with very different force characteristics, i.e.
with NRL allergy into two phases: ‘pre-treatment’ and
nickel titanium springs, elastics and Bennett modules,
‘during treatment’. The salient features can be incorpo-
still found each method to be clinically effective.19–21 So,
although NRL-free elastics do not perform as well asNRL elastics in laboratory studies, it is unlikely that the
relatively small mechanical differences in force decaywould have a clinically significant effect. No clinical trial
Synthetic non-latex gloves are readily available for
has compared NRL and NRL-free elastics to date.
clinical use, and include gloves made from nitrile,polychloroprene, elastyren and vinyl. The developmentand marketing of new gloves is a rapidly changing and
competitive area. The choice of gloves is based on
operational need and personal preference. The clinician
needs to consider the level of comfort, the degree of
The management will depend on the severity of the
dexterity required by a procedure, the infection risk, and
patient’s reaction, which may range from contact
the potential for allergic and other adverse reactions to
urticaria (CU) to full-blown anaphylaxis. CU is managed
gloves. All gloves, irrespective of the presence of latex,
by avoiding any contact with NRL and possibly
must meet the European standard for single-use medical
administering an oral antihistamine such as chlorphena-
gloves. Poley and Slater reported that the vinyl gloves
mine. The patient needs to be warned of the likelihood of
available at the time had higher in-use leakage rates.7
drowsiness if a sedating antihistamine is used, and may be
However, vinyl examination gloves for medical use that
sent home accompanied after a few hours of observation.
meet current glove standards are now available.16
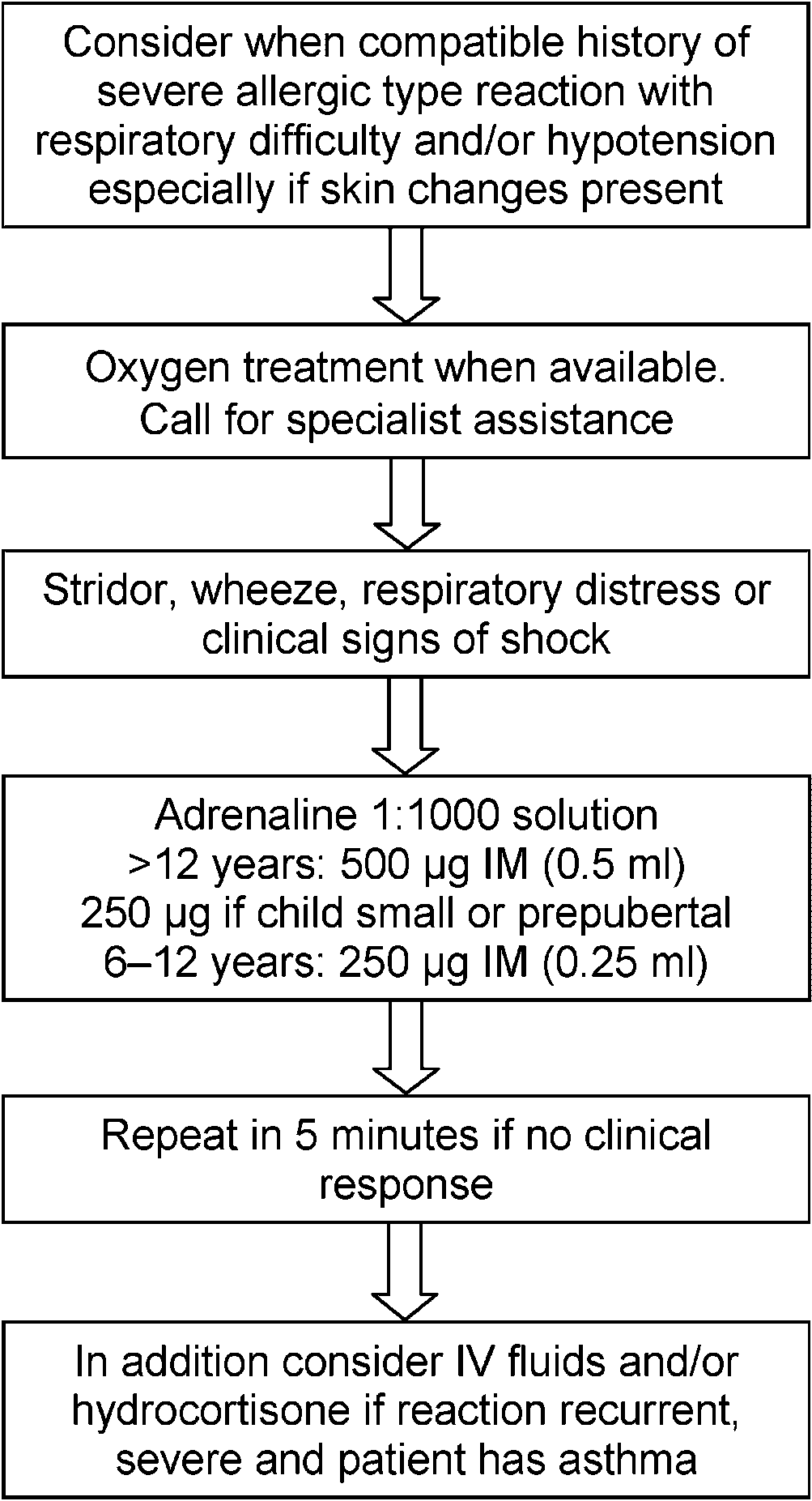
A diagnosis of anaphylaxis can be made in the
presence of respiratory distress and or hypotension.
However, time should not be wasted in applying strictcriteria in a deteriorating patient, and adrenaline should
NRL is commonly found in the dental surgery and in a
be given early (IM). The administration of salbutamol,
number of orthodontic materials. Table 1 lists NRL-free
chlorphenamine and hydrocortisone should also be
alternatives to commonly used orthodontic materials
and products that may contain NRL. Consideration,however, should also be given to general items of dentalequipment that may be required, such as rubber
polishing cups, alginate mixing bowls and local anaes-
Concerns about the mechanical properties of NRL-
Owing to the frequent contact with NRL, dental HCWs
free elastics used in orthodontics have been raised.4 The
are at increased risk of developing NRL allergy.14 The
extension force pattern was reported to be different for
Health and Safety Act 1974 requires employers to take
NRL and NRL-free alternatives.4,17 Silicone bands also
all reasonable steps to ensure the welfare of their
be sought from the local cccupational health service(OHS) about the advisability of the staff memberworking in dentistry. If an HCW develops signs orsymptoms of NRL allergy, they should contact an OHSphysician so that investigations can be arranged and adiagnosis established. Fortunately, most cases of low-grade hand dermatitis are irritant rather than allergicand respond to a change in hand care regime.16 If adiagnosis of NRL allergy is made, the safety of theworking environment needs to be reviewed. If symptomspersist despite all attempts to provide a safe workenvironment, then relocation of the employee needs tobe considered. It is a statutory duty of the employer tokeep records of occupational dermatitis attributableto NRL and report these to the Health and SafetyExecutive. Adverse Reaction to Dental Materials canalso be registered online at http://arrp.group.shef.ac.uk.
NRL allergy is a significant clinical problem withpotentially life-threatening complications. Risks can beminimized by:
N taking an up-to-date medical history;N arranging investigations for patients with a suspected
NRL sensitivity/allergy and ensuring that the patientis referred to an appropriate medical specialist;
N treating patients with a suspected or proven NRL
allergy in a ‘latex-screened’ environment;
N selecting NRL-free orthodontic products;N recognizing acute symptoms of NRL allergy and
instigating prompt emergency treatment.
Appendix 1: Checklist for patients withNRL allergy
Anaphylactic reactions: treatment algorithm (adapted
N Identify a member of staff to implement ‘NRL allergic
employees. As NRL comes under Control of Sub-
stances Hazardous to Health Regulations 1999, the
N Ensure that all staff are aware of implication of
employer is expected to institute preventive measures to
control the risks posed by NRL. Employers are there-
N A sign on the surgery door should indicate ‘latex-
fore expected to ensure that NRL gloves are only used if
there is an operational need, that powdered gloves are
N Case notes should be clearly marked to warn staff.
not used and that only gloves with low leachable protein
N The latex-screened zone should be decontaminated
are made available for use. A protocol should also be
available covering the protection of sensitive HCWs and
N NRL products must not be stored in the latex-
the management of patients with NRL allergy.
screened surgery or with the NRL-free items.
Ideally, prospective employees should be screened for
N Staff should wear fresh protective clothes, and
NRL allergy before they are employed. Advice can then
N Any facemasks should have paper ties.
reactions to natural rubber latex: results of a multicentre
N Have NRL-free emergency equipment at hand.16
study. Br J Dermatol 2002; 146 :114–17.
N Discuss all aspects of treatment with the patient.
11. Neiburger EJ. A case of possible latex allergy. J Clin Orthod
N Ensure that all personnel, for example radiographers
or new staff likely to come into contact with the
12. Everett FG, Hice TL. Contact stomatitis resulting from the
patient, are aware of the NRL allergy.
use of orthodontic rubber elastics: report of case. J Am DentAssoc 1974; 88: 1030–31.
13. Shoup AJ. Guidelines for the management of latex allergies
and safe use of latex in perioperative practice settings. AORN J 1997; 66: 726, 729–31.
N All equipment must be NRL-free (see Table 1).
14. Saary MJ, Kanani A, Alghadeer H, Holness DL, Tarlo SM.
NB: Powdered NRL gloves should not be used in a
Changes in rates of natural rubber latex sensitivity among
dental school students and staff members after changes inlatex gloves. J Allergy Clin Immunol 2002 ;109: 131–35.
15. Field EA, Fay MF. Issues of latex safety in dentistry. Br
16. Field EA, Longman LP. Guidance for the Management of
1. Jacobsen N, Hensten-Pettersen A. Changes in occupational
Natural Rubber Latex Allergy in Dental Patients and Dental
health problems and adverse patient reactions in orthodon-
Health Care Workers. London: Faculty of General Dental
tics from 1987 to 2000. Eur J Orthod 2003; 25: 591–98.
Practitioners (UK), The Royal College of Surgeons, 2004.
2. Snyder HA, Settle S. The rise in latex allergy: implications
17. Hwang CJ, Cha JY. Mechanical and biological comparison
for the dentist. J Am Dent Assoc 1994; 125(8): 1089–97.
of latex and silicone rubber bands. Am J Orthod Dentofacial
3. Hanson M, Lobner D. In vitro neuronal cytotoxicity of
latex and non-latex orthodontic elastics. Am J Orthod
18. Ren Y, Maltha JC, Kuijpers-Jagtman AM. Optimum force
Dentofacial Orthop 2004; 126(1): 65–70.
magnitude for orthodontic tooth movement: a systematic
4. Russell KA, Milne AD, Khanna RA, Lee JM. In vitro
assessment of the mechanical properties of latex and non-
literature review. Angle Orthod 2003; 73: 86–92.
latex orthodontic elastics. Am J Orthod Dentofacial Orthop
19. Samuels RH, Rudge SJ, Mair LH. A clinical study of space
closure with nickel–titanium closed coil springs and an
5. Nattrass C, Ireland AJ, Lovell CR. Latex allergy in an
elastic module. Am J Orthod Dentofacial Orthop 1998; 114:
orthognathic patient and implications for clinical manage-
ment. Br J Oral Maxillofac Surg 1999; 37: 11–13.
20. Nightingale C, Jones SP. A clinical investigation of force
6. Everett FG, Hice TL. Contact stomatitis resulting from the
delivery systems for orthodontic space closure. J Orthod
use of orthodontic rubber elastics: report of case. J Am Dent
21. Dixon V, Read MJ, O’Brien KD, Worthington HV,
7. Poley GE Jr, Slater JE. Latex allergy. J Allergy Clin
Mandall NA. A randomized clinical trial to compare three
methods of orthodontic space closure. J Orthod 2002; 29:
8. Cullinan P, Brown R, Field A, et al. Latex allergy. A
position paper of the British Society of Allergy and Clinical
Immunology. Clin Exp Allergy 2003; 33: 1484–99.
Emergency Medical Treatment of Anaphylactic Reactions
9. Wakelin SH, White IR. Natural rubber latex allergy. Clin
for First Medical Responders and the Community Nurses.
Published 1999; revised 2002 and 2005. Available at:
10. Sommer S, Wilkinson SM, Beck MH, English JS,
http://www.resus.org.uk/pages/reaction.htm (accessed 21
Gawkrodger DJ, Green C. Type IV hypersensitivity
REVITALISASI DAN PEMANFAATAN BENTENG VREDEBURG DI YOGYAKARTA TAHUN 1976 – 2011 Soma Harjad Prasetya C0506050 Abstract Vredeburg Castle originally named "Fort Rustenburg" having meaning "Castle Rest". Vredeburg Castle is a Dutch Colonial heritage even in very simple form with the development of the castle still remain standing and functional. Since the found
Estatuto do Jornalista Publicada em 13 de Janeiro de 1999, a lei fundamental para o exercício da profissão de jornalista define a respectiva actividade, normas de acesso à profissão, direitos e deveres dos jornalistas, acesso às fontes e sigilo profissional, entre outros aspectos. Foi alterada pela Lei n.º 64/2007, de 6 de Novembro, com rectificações feitas pela Declaração de Rect
 be sought from the local cccupational health service(OHS) about the advisability of the staff memberworking in dentistry. If an HCW develops signs orsymptoms of NRL allergy, they should contact an OHSphysician so that investigations can be arranged and adiagnosis established. Fortunately, most cases of low-grade hand dermatitis are irritant rather than allergicand respond to a change in hand care regime.16 If adiagnosis of NRL allergy is made, the safety of theworking environment needs to be reviewed. If symptomspersist despite all attempts to provide a safe workenvironment, then relocation of the employee needs tobe considered. It is a statutory duty of the employer tokeep records of occupational dermatitis attributableto NRL and report these to the Health and SafetyExecutive. Adverse Reaction to Dental Materials canalso be registered online at http://arrp.group.shef.ac.uk.
be sought from the local cccupational health service(OHS) about the advisability of the staff memberworking in dentistry. If an HCW develops signs orsymptoms of NRL allergy, they should contact an OHSphysician so that investigations can be arranged and adiagnosis established. Fortunately, most cases of low-grade hand dermatitis are irritant rather than allergicand respond to a change in hand care regime.16 If adiagnosis of NRL allergy is made, the safety of theworking environment needs to be reviewed. If symptomspersist despite all attempts to provide a safe workenvironment, then relocation of the employee needs tobe considered. It is a statutory duty of the employer tokeep records of occupational dermatitis attributableto NRL and report these to the Health and SafetyExecutive. Adverse Reaction to Dental Materials canalso be registered online at http://arrp.group.shef.ac.uk.