Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Doi:10.1016/s0006-3223(02)01740-7
Diurnal Variation of Cerebrospinal Fluid Hypocretin-1(Orexin-A) Levels in Control and Depressed Subjects
Ronald M. Salomon, Beth Ripley, John S. Kennedy, Benjamin Johnson,Dennis Schmidt, Jamie M. Zeitzer, Seiji Nishino, and Emmanuel Mignot
Background: Hypocretins, excitatory neuropeptides at Introduction monoaminergic synapses, appear to regulate humansleep-wake cycles. Undetectable cerebrospinal fluid hypo-
Among pathophysiologic findings in depression, rela-
cretin-1 levels are seen in narcolepsy, which is frequently
tionships with sleep and circadian abnormalities have
associated with secondary depression. Shortened rapideye movement latency is observed in both narcolepsy anddepression. Cerebrospinal fluid hypocretin-1 levels havenot been reported in mood disorders.
early in the course of the disease include sleep distur-
Methods: We examined hypocretin-1 levels in 14 control and 15 depressed subjects. Cerebrospinal fluid was drawn
especially rapid eye movement (REM) deprivation have
continuously in supine subjects for 24 hours with anindwelling intrathecal catheter under entrained light-darkconditions. Depressed subjects were studied before andafter 5 weeks of sertraline (n ϭ 10, three nonresponders)or bupropion (n ϭ 5, two nonresponders).
and decreased REM latency in depression is highly
Results: Hypocretin-1 levels varied slightly (amplitude 10%) but significantly across the diurnal cycle in control
creased amplitudes of behavioral, physiologic, and neu-
subjects, with amplitude significantly reduced in depres-
roendocrine circadian measures and disrupted responses of
sion (3%). Levels were lowest at midday, surprising for ahypothetically wake-promoting peptide. Mean hypocretin
the circadian pacemaker to the light-dark cycle are ob-
levels trended higher in depressive than in control sub-jects. Hypocretin-1 levels decreased modestly but signifi-cantly after sertraline (Ϫ14%) but not bupropion.Conclusions: Our results are consistent with previous phys-
sion is associated with diurnal changes in hypothalamic-
iologic findings in depression indicating dampened diurnal
pituitary-adrenal axis activity and other endocrine abnor-
variations in hypocretin-1. The finding that sertraline but notbupropion slightly decreased cerebrospinal fluid hypocre-tin-1 indicates a serotoninergic influence on hypocretin tone.
Biol Psychiatry 2003;54:96 –104 2003 Society of Biolog-
hypocretin-1 and hypocretin-2, are processed from aprepropeptide encoded by a single gene
Key Words: Depression, hypocretin, sertraline, bupro-
tuberal region of the hypothalamus project to the entire neuraxis, including the spinalcord Extremely dense and almost
From the Department of Psychiatry (RMS, DS) and Anesthesiology (BJ), Vander-
bilt University School of Medicine, Nashville, Tennessee; the Stanford Uni-
invariably excitatory projections are noted to aminergic
versity Center for Narcolepsy (BR, JMZ, SN, EM), Stanford University School
cell groups (e.g., adrenergic locus coeruleus, serotonergic
of Medicine, Palo Alto, California; the Department of Psychiatry (JSK),Indiana University School of Medicine and Lilly Research Laboratories, Eli
raphe´ nuclei, histaminergic tuberomammillary nucleus,
Lilly and Company (JSK), Indianapolis, Indiana.
dopaminergic substantia nigra, and ventral tegmental area;
Presented in part in meeting abstract at the annual conference of the Associated
Professional Sleep Societies, Seattle, Washington, June 2002.
Address reprint requests to Ronald M. Salomon, Vanderbilt University School of
Medicine, Department of Psychiatry, VAV 2200, 1500 21st Ave S, Nashville,TN 37212, or to Emmanuel Mignot, M.D., Ph.D., Stanford University Center
for Narcolepsy, 701 Welch Road B, basement room 145, Palo Alto, CA
ment links transmitter systems of each of the respective
Received April 23, 2002; revised August 7, 2002; accepted September 4, 2002.
nuclei to the pathophysiology of depression (Janowsky
and Overstreet 1995; Maes and Meltzer 1995; Schatzberg
ter (GCRC) from 1990 to present. Patients showing any sugges-
tion of less than optimal cognition and thought processes were
excluded because of inability to provide consent. Additionally,
seven healthy subjects (four of them male, 27.7 Ϯ 4.86 years old)
a disabling disorder characterized by daytime sleepiness,
were studied repeatedly on separate days at different hours acrossthe day and night with standard lumbar puncture procedures with
cataplexy, and extremely short REM sleep latency
the approval of the Stanford University institutional review
At the Vanderbilt University site, subjects were recruited by
and may consolidate wakefulness and reduce sleep. Mono-
newspaper advertisement. Depressed patients were in medically
aminergic tone, which is high during wakefulness, de-
stable condition, were 18 to 65 years old, had a DSM-IV major
creases during sleep and REM sleep and may be driven by
depressive episode, and had been free of antidepressant drugs for
at least 2 months. Exclusion criteria included high suicidal risk
(e.g., previous severe suicide attempt), past or present psychosis,
reduce monoaminergic activity, leading to daytime sleep-
current tobacco use, and the existence of any other primary
iness and abnormally short REM sleep latency
psychiatric diagnosis. Subjects were also free of abnormalities on
physical examination, electrocardiogram, or extensive laboratory
Narcolepsy is frequently associated with depression
evaluation (including hepatitis screens and pregnancy testing). Eligibility required agreement from the subject to comply with
all study requirements. All subjects were reimbursed for incon-
enhance monoaminergic activity and affect sleep physiol-
venience and expenses and income lost, and depressed patients
ogy. The hypocretin system is activated by sleep (or REM)
received free treatment for 8 study weeks. In the case of the
limited number of healthy volunteers studied at Stanford Uni-
antidepressant effects Finally, hypocretins
versity, subjects were recruited by word of mouth, compensated
activate the hypothalamic-pituitary-adrenal axis
for their effort, and included only if they were free of any
medical illness and psychotropic treatment.
These relationships led us to study the role of hypocretins
At both sites the study and potential risks were fully explained
in depression. To do so we examined lumbar cerebrospinal
and all questions were answered before informed consent was
fluid (CSF) hypocretin-1 levels in 14 control and 15
signed, typically after several days of consideration by the
depressed subjects (before and after antidepressant ther-
subject along with family members and close friends. Discomfort
and inconvenience, most notably spinal headache, and potentialrisk for serious adverse outcomes, such as the potential forparalysis or death as a result of treatment-resistant bacterialmeningitis resulting from participating in the CSF collection
Methods and Materials
procedure, were all thoroughly discussed.
Fourteen control subjects (six of them male, 41 Ϯ 4 years old [allexpressions are mean Ϯ SD]) and 15 depressive subjects (five of
In the continuous 24-hour CSF sampling studies, healthy subjects
them male, 39 Ϯ 3 years old) were studied with continuous CSF
were studied on only one occasion, whereas depressed subjects
sampling. Diagnosis was determined by psychiatric interview
were studied before and after 5 weeks of antidepressant therapy
and confirmed by the Structured Clinical Interview for DSM-IV
with sertraline (n ϭ 10, three nonresponders) or bupropion (n ϭ
Axis I Disorders and Structured Clinical Interview for DSM-IV
5, two nonresponders). All subjects consumed a controlled,
Axis II Disorders according to DSM-IV
balanced monoamine diet provided by the outpatient GCRC for
three daily meals for 3 days before each catheterization. During
item Hamilton Rating Scale for Depression (HRSD) score was
the entire preadmission and inpatient study, subjects were not
permitted to consume methylxanthine-containing foods, such as
subjects with bipolar type I, four with bipolar type II, and others
caffeinated beverages, chocolate, and artichokes. Diets were
with unipolar illness or a first depressive episode (one patient).
designed by the nutritionist according to individual taste prefer-
On average, patients described 2.5 discrete depressive episodes,
ences to maximize compliance. Balanced meals contained ap-
although this may be a low estimate because many episodes were
proximately 50% carbohydrates, 20% protein, and 30% fat. On
described as prolonged and thus may have represented several in
admission into the GCRC, meals were given only at 6:30 AM and
series without full interepisode recovery, and most patients
9:30 AM, yielding the same total daily intake. All subjects
described onset early in life with only recent diagnosis. None had
remained strictly supine during the precatheterization (12 hours),
illness considered refractory to treatment in previous episodes.
catheterization (48 hours), and postcatheterization (24 hours)
The studies were approved by the Vanderbilt University institu-
periods and were not allowed to rise for any reason (including
tional review board and the committee of the National Institutes
being required to toilet in the supine position). Thus the total time
of Health–supported Vanderbilt General Clinical Research Cen-
that each subject was required to be recumbent in bed was a
Table 1. Depressed Patient Protocol and Rating Scale Results
For physical symptom checklist, baseline symptoms were rated before first CSF study as 1, none or negligible; 2, mild; 3, moderate; 4, severe. There was no clinically
or statistically significant worsening during the study from baseline at any point, although there were frequently significant improvements.
minimum of 84 hours for each of the two sampling periods. After
screening and initial GCRC intake scores at week 8 of treatment
the 24-hour baseline period reported here, participants received
(study week 10), and (2) an HRSD total score at the final week
dietary restrictions or medications for other study purposes;
8 assessment of 8 or less. According to these criteria, only five of
however, the second 24-hour collection period is not relevant to
15 subjects were nonresponders, three with sertraline and two
this report. Patients were encouraged to change position fre-
quently. Room lights were turned off at 11:00 PM and back on at6:15 AM before breakfast at 6:30 AM. CSF collection was adapted
Monitoring of Side Effects and Adverse Events
from a previously reported procedure Forhealthy subjects, intrathecal catheters were placed at 6:00 PM,
Weekly outpatient and twice-daily inpatient ratings for study-
and collection began at 6:30 PM. For depressed subjects, intra-
related adverse events were recorded and analyzed. There was no
thecal catheters were in place by 7:30 AM, and collections began
statistically or clinically significant worsening relative to base-
at 8:00 AM. CSF samples were collected into polypropylene vials
line physical symptom checklist, which included headache,
held in a chilled fraction collector at 4°C and moved to dry ice at
constipation, poor memory, nausea, drowsiness, blurred vision,
increased appetite, difficulty starting urination, trouble concen-
In a separate study, seven healthy subjects had lumbar punc-
trating, nightmares, difficulty sitting still, irregular heartbeat,
tures in the early afternoon, the middle of the night, and the early
diarrhea, frequent urination, dry mouth, decreased appetite,
morning, with samplings being separated by at least 2 weeks.
tremors or shakiness, skin rash, ringing in ears, sweating, fainting
Subjects were instructed to continue their normal activity sched-
or light-headedness, poor muscle coordination, and muscle stiff-
ule and were allowed to sleep in the laboratory in preparation for
ness. A total physical symptom checklist score was also gener-
their nocturnal and early morning spinal taps. Not all subjects
ated and did not vary across the study although a small
completed all three studies because of headaches (n ϭ 3) or other
improvement was noted in treated depressed subjects (data not
intervening circumstances (n ϭ 3).
shown). Importantly, there were also no time points with groupdifferences for headache. Three days after withdrawal of the CSFcatheter, all depressed subjects were free of headache. Most
Antidepressant Treatment and Definition of
subjects had extremely limited symptom changes through the
course of the study. Severe headaches were unusual, any head-
As shown in depressed patients were assigned to 8
ache was infrequent, and all postspinal headaches resolved with
weeks of open-label, outpatient treatment with either sertraline
a local blood patch administered between 24 and 72 hours after
(Zoloft, all of the first five patients plus five randomly assigned
the catheter removal. A blood patch procedure was offered and
of the other 10 depressed subjects) or bupropion (Wellbutrin-XR,
performed after seven of the 30 catheterizations that were
all five randomly assigned). Antidepressant treatment was initi-
ated in the morning of the third day after the completion ofpretreatment lumbar intrathecal catheterization. All patients were
free of spinal headaches before beginning therapy and reportedtaking all their medications. Sertraline therapy began with 50 mg
CSF hypocretin-1 levels were measured in duplicate with an
each morning for 7 days and increased to 100 milligrams each
established direct radioimmunoassay in 10-min samples (50 L
day for 7 weeks. Bupropion was given as extended release
ϫ 2; The CSF hypocretin-1 assay was highly
150-mg tablets each morning for the first 7 days and then 150
reliable, showing stability in samples measured repeatedly from
milligrams each morning and each day at 1:00 PM for 7 weeks.
samples kept frozen (Ϫ80°C) for as long as 10 years, after 72
The HRSD was the primary mood outcome measure. An
hours at room temperature, or repeatedly thawed and frozen
HRSD decrease of 50% or reaching 8 or less defined remission
Specificity was shown (r ϭ .99, p Ͻ .001)
at 5 weeks. After 8 weeks of treatment, end point remission was
by linear correlation of exogenous hypocretin-1 (0 –1200 pg/mL)
defined similarly as meeting both a priori criteria: (1) decrease on
in 1 mL CSF to the obtained level measurements
the HRSD total score of at least 50% from the mean of HRSD
Measured levels were at least 15 times greater than
Table 2. Sinusoidal Curve Fitting in Control and Depressed Subjects
Data are mean Ϯ SD. Times are given as 24-hour clock times.
minimal detectable levels In 11 subjects (six
.001). Contrary to an expected increasing level gradient
control subjects and five depressed subjects before and after
across serial samples that is often reported in monoamine
treatment), all samples were assayed. In the remaining eight
metabolite measures, levels of hypocretin declined very
control subjects and 10 depressed (before and after) subjects, one
gradually during the first few hours of sampling (average
8.8% in 3.5 hours). This differs from the monoamineeffect in that our opening fluid samples were reserved for
culture and microscopy as part of a safety procedure, and
To study overall diurnal variation, data smoothing was per-
the hypocretin gradient was observed over a longer period.
formed by averaging 10-min hypocretin-1 values across 2 hour
Sinusoid curve-fitting results are indicated in and
periods. Data were normalized within subjects by dividing each
A 24-hour sine wave accurately predicted the
data point by the mean 24-hour hypocretin value of the subject
form of the data from control subjects (r2 ϭ .92), with an
and then averaging across subjects within treatment groups.
amplitude of 6% and a peak occurring several hours after
Group data were fitted with a 24-hour cosine-wave function (y ϭ
a ϩ {b ϫ cos[(2/24) ϫx ϩ c]}) with a nonlinear, least-squares
depressed subjects, both before and after treatment, a sine
fitting method (Levenberg-Marquardt algorithm, Microcal Ori-
wave poorly predicted the overall oscillation of lumbar
gin v.6.0; Microcal Software, Northampton, MA). The phases of
hypocretin (r2 ϭ .32 before treatment, r2 ϭ .42 after
hypocretin maxima and hypocretin fluctuation amplitude (half
treatment), and the amplitude of wave was apparently
peak to trough) were estimated for each group.
Daytime and nighttime values were also compared. In each
reduced, with nonoverlapping 95% confidence intervals
individual subject mean hypocretin levels during the day
between control subjects and depressed subjects before or
(11 AM– 6:00 PM) and night (11 PM– 6:00 AM) were calculated,
after treatment. There may have been a small recovery of
together with mean 24-hour individual hypocretin-1 levels. The
amplitude in the depressed patients after treatment, though
7-hour day and night windows were selected according to
such an effect is not statistically evident from the sine-
light-dark schedule (lights were off from 11 PM– 6:00 AM).
fitting data. In an additional limited set of ambulatory
Day-night differences in mean levels (11 PM– 6:00 AM minus
control subjects who underwent multiple lumbar punctures
11AM– 6:00 PM) for each subject were considered an approxima-tion of the amplitude on each experimental night. We compareddaytime and nighttime hypocretin levels within each of the threesubject groups (two-tailed, paired Student t tests), daytime andnighttime levels, and day-night differences between groups(single-factor ANOVA) and the effect of antidepressant treat-ment (two-factor ANOVA). Statistical analyses were performedon a personal computer with Excel 2000 (v. 9.0.2720; MicrosoftCorporation, Redmond WA), with the exception of the two-factor ANOVAs that were performed with the Java script foundon http://faculty.vassar.edu/lowry/anova2u.html
Diurnal Variation of Hypocretin-1 Levels inDepressed and Control Subjects
Overall the concentration of hypocretin-1 obtained fromhuman lumbar CSF did not vary significantly with age or
Figure 1. Sinusoidal fitted curves to 2-hour interval measure-
gender (not shown), in agreement with previous reports. In
ments of CSF hypocretin-1 levels from lumbar catheterization in
control subjects, hypocretin levels varied very slightly but
control (squares), depressed (triangles), and treated (circles)
consistently and significantly across the diurnal cycle (p Ͻ
Basal Levels of Hypocretin-1 in Depressed andControl Subjects
Basal 24-hour, daytime, and nighttime levels did not differbetween supine control subjects and untreated patients, butslightly higher levels were observed in depressed subjects,especially during the day (daytime concentrations in con-trol subjects 251.7 Ϯ 11.5 pg/mL and in pretreatmentdepressed subjects 275.8 Ϯ 11.5 pg/mL, nighttime con-centrations in control subjects 274.0 Ϯ 10.6 pg/mL and inpretreatment depressed 280.9 Ϯ 12.2 pg/mL, mean-24hour concentrations in control subjects 265.0 Ϯ 11.0pg/mL and in pretreatment depressed subjects 281.2 Ϯ11.8 pg/mL, differences not significant; Thesevalues were also similar to previously reported data inambulatory control subjects and markedly higher thanlevels observed in narcolepsy. As suspected from thesinusoid analysis, there was a highly significant differencebetween daytime (11:00 AM– 6:00 PM) and night time(11:00 PM– 6:00 AM) hypocretin-1 concentrations in con-trol subjects (p Ͻ .001, paired two-tailed t test). Theday-night difference was lost in depressive subjects before(p ϭ .32, paired two-tailed t test) or after (p ϭ .24, pairedtwo-tailed t test) treatment. Effects of Antidepressant Treatment on Hypocretin-
Figure 2. Seven healthy volunteers had spinal taps at different
times of the day, with five of them having at least two taps atdifferent times of the day (singleton values not shown). Symbols
Drug effects were associated with changes in hypocretin
connected by solid lines indicate the concentration of hypocre-
levels, whereas mood responses were not. Hypocretin
tin-1 (Hcrt-1) in the CSF of single spinal taps for each individual.
levels decreased modestly but significantly both overall
Multiple samplings in the same individual are connected with
with sertraline treatment: (Ϫ14%, p Ͻ .01), both during
solid lines. The averages of the samples obtained in the early
the day (Ϫ14%, p Ͻ .05) and during the night (Ϫ14%,
afternoon, early night, and late night are shown as diamonds,
p Ͻ .005) but not with bupropion treatment: (overall
with x and y axis error bars representing SEM, and are connected
Ϫ3%, p ϭ .59; daytime Ϫ4%, p ϭ .35; nighttime Ϫ1%,
by a dashed line. The time of day is indicated on the x axis, and
p ϭ .91; all p values from two-tailed, paired t tests;
the dark period is approximated by the black bar (10:00 PM–
Absolute concentrations of hypocretin during the day,
night, or 24-hour sampling period, as well as the differ-ence between day and night (a measure of circadian
at different times of day, levels did not vary significantly
amplitude), were affected neither by treatment nor out-
but were generally slightly higher during the nighttime,
come (two-factor ANOVA p Ͼ .38 for all comparisons
in agreement with the continuous sampling data set
and interactions; Pretreatment to posttreatment
changes in hypocretin concentrations during the day,
Table 3. Mean Ϯ SEM Hypocretin Levels in Control Subjects and Depressed Patients before and after Treatments
There were significant differences (p Ͻ .05) between depressed and control groups and in depressed group before and after treatment as indicated. aSignificant difference between depressed and control group by t test. bSignificant difference between before and after treatment by paired t test.
Table 4. Mean Ϯ SEM Hypocretin Levels (in picograms per milliliter) in Depressed Patients and Treatment Responses
aSignificant (p Ͻ .05, paired t test) effects from pretreatment to posttreatment. bSignificant (p Ͻ .05, paired t test) drug effects from pretreatment to posttreatment.
night, or 24-hour sampling period were also not affected
part of the active day period, just before the transition to
by treatment or outcome (two-factor ANOVA p Ͼ .05 for
tion that hypocretin may be an important wake promotingsignal, opposing sleep debt in the second part of the activephase
Discussion
In our human lumbar CSF study, highest values
This study presents data from subjects confined to bed rest
were observed around 2:00 AM (3 hours after lights out),
for 12 hours before the lumbar puncture and also from
which is several hours later than in the squirrel monkey.
subjects allowed ad libitum activity until the time of the
Furthermore, changes were of much smaller magnitude
lumbar puncture. Under condition of constant bed rest,
than in the nonhuman mammalian studies. This temporal
continuously sampled (for 24 hours) CSF hypocretin-1
difference most likely reflects an anatomically delayed
levels fluctuated moderately but significantly across the
and dilution-dampened oscillation of cortical hypocretin,
24-hour cycle (Ͻ15%; Similar variations were
with actual brain fluctuations being more consistent with
observed in the small number of subjects in the individual
the monkey data. Consistent with this hypothesis, studies
tap study indicating that normal activity did not
have shown a 90- to 120-minute delay in equilibration
dramatically alter this profile. The observation that fluc-
between higher CSF compartments and the lumbar sac
tuations in levels across the 24-hour period were much
smaller than differences observed between groups of
Intense projections from the hypothalamus to the spinal
healthy and narcoleptic patients is of practical importance.
cord have been reported (van den Pol 1999), but even if
Lower CSF hypocretin levels (hypocretin-1 levels Ͻ110
spinal release occurs, the cell bodies located in the lateral
pg/mL) have been shown to be diagnostic for narcolepsy
hypothalamic area are likely to be active during the active
period. This would not explain the discrepancy between
indicate that the time of day at which sampling is done is
unlikely to interfere with this test. The data should be
Hypocretins are uniquely positioned for involvement in
considered preliminary because of the relatively small
depression. Whereas hypocretin cell bodies are all local-
number of patients and the differences in times of collec-
ized within the perifornical area, extremely dense, almost
tion initiation between control subjects and depressed
invariably excitatory projections are noted in aminergic
cell groups (e.g., adrenergic locus coeruleus, serotonergic
Surprisingly, the direction of the hypocretin diurnal
raphe´ nuclei, histaminergic tuberomammillary nucleus,
variation observed in the CSF was opposite to that
dopaminergic substantia nigra, and ventral tegmental area
expected for a wake-promoting peptide. Highest levels
were observed in the middle of the night, while subjects
were mostly asleep. In rats, both cisternal CSF
have reported higher levels in the latter portion of
hypocretin system in narcolepsy was first demonstrated in
the active phase (dark period). In diurnal squirrel monkeys
(Saimiri sciureus), cisterna magna CSF levels of hypocre-
Hypocretin deficiency causes human narcolepsy
tin (ranging from 170 – 430 pg/mL, similar to the human
samples) were also found to be highest during the latter
disabling disorder characterized by daytime sleepiness,
cataplexy, and extremely short REM sleep latency
with decreased hypocretin levels, suggesting a small but
significant serotonergic influence on hypocretin tone after
5 weeks of treatment. The finding that bupropion, a
Hypocretin release is higher during the active phase in rats
dopaminergic and adrenergic reuptake blocker with sig-
not modify hypocretin levels was rather surprising. The
Whereas decreased hypocretin tone in narcolepsy is
fact that sertraline is a more potent REM-suppressing
associated with depression, our data indicate no dramatic
decrease in baseline CSF hypocretin values in depression.
significant in explaining this difference. Alternatively,
If anything, slightly higher hypocretin values were found
changes caused by bupropion may be observed either
in this small number of depressed subjects This
acutely, after initial dosing, or more delayed in recovery.
finding indicates that hypocretin deficiency is an unlikely
Stimulant medications such as amphetaminelike dopamine
cause for depression. Slightly increased hypocretin levels
releasing agents and reuptake inhibitors have not dramat-
in depression may rather represent disturbed sleep and
ically modified CSF hypocretin levels in patients with
activity in depression or compensatory mechanisms. Stud-
ies with larger numbers are, however, needed to expand on
acute changes in hypocretin are observed in preclinical
studies of dopamine releasing agents. Studies including
In contrast with the lack of striking baseline hypocretin
narcoleptic subjects treated with serotonin reuptake inhib-
level differences, we found significantly decreased diurnal
itors may be needed to study this effect.
variation in depressed subjects versus control subjects.
In conclusion, our studies of CSF hypocretin-1 levels in
These results are consistent with previous findings in
depression indicate that a decrease in mean hypocretin
depression indicating that diurnal physiologic measures
release is not a likely cause of depression. In control
subjects, CSF hypocretin-1 levels were found to vary
slightly but significantly across the 24-hour study period,
source of the observed diminution in signal amplitude
with higher levels observed at night. In depression, re-
cannot be ascribed definitively to any of the involved sites.
duced amplitude of diurnal variation was observed. Addi-
This observation does, however, provide evidence in
tional studies in depression are needed to expand on these
depression that diminished circadian rhythms of behav-
iors, physiologic measures, and peripheral neuroendocrinefunctions can also be observed centrally. Evidence sug-gests dampened monoamine metabolite fluctuation in
Supported by grants from the National Institutes of Health (Grants NS
depression (Salomon et al 1998, unpublished data). Sleep
23724, NS 33797, and MH40041) to EM, by an investigator-initiatedgrant from Pfizer, by grants from National Alliance for Research in
Schizophrenia and Depression and the Theodore and Vada Stanley
caused by decreased hypocretin fluctuation. Interestingly,
Foundation to RMS, and by a General Clinical Research Grant from the
however, relief of depressive symptoms was not correlated
National Institutes of Health National Center for Research Resources
with restored diurnal rhythmicity in this small sample.
(Grant MO1RR00095) to Vanderbilt University Medical Center, Nash-
Still, a slight improvement in amplitude was noted in
We thank our research assistants, Linda Todd, Barbee Smith, and
treated subjects. This is highly vulnerable to error because
Kerry Hook, the General Clinical Research Center nursing staff, and all
of the small sample size and the relatively mild to
moderate depressive episodes in these patients and thuswill require replication; however, our results suggest thatdepressive mood and diurnal variation in hypocretins may
References
be independent characteristics. Chronic treatment studies
American Psychiatric Association (1994): Diagnostic and Sta-
in depression may lead to more significant changes in
tistical Manual of Mental Disorders, 4th ed. Washington, DC:
hypocretin diurnal variation, especially if the restoration of
sleep patterns from direct soporific effects is avoided and
Arborelius L, Owens MJ, Plotsky PM, Nemeroff CB (1999): The
the delayed normalization of sleep is related to peptidergic
role of corticotropin-releasing factor in depression and anxi-ety disorders. J Endocrinol 160:1–12.
Benca RM, Obermeyer WH, Thisted RA, Gillin JC (1992): Sleep
We also explored whether antidepressant treatment
and psychiatric disorders. A meta-analysis. Arch Gen Psychi-
modified CSF hypocretin levels in patients with depres-
sion. A possible pharmacologic effect not related to
Beersma DG, Van den Hoofdakker RH, Van Berkestijn JW
antidepressant response was observed. We found that
(1983): Circadian rhythms in affective disorders. Body tem-
treatment with sertraline but not bupropion was associated
perature and sleep physiology in endogenous depressives. In:
Van Praag HM, Mendlewicz J, editors. Advances in Biolog-
Jaszberenyi M, Bujdoso E, Pataki I, Telegdy G (2000): Effects of
ical Psychiatry, 11. Basel: Karger, 114 –127.
orexins on the hypothalamic-pituitary-adrenal system. J Neu-
Beuckmann CT, Yanagisawa M (2002): Orexins: From neu-
roendocrinol 12:1174 –1178.
ropeptides to energy homeostasis and sleep/wake regulation.
Kennedy JS, Polinsky RJ, Johnson B, Loosen P, Enz A,
Laplanche R, et al (1999): Preferential cerebrospinal fluid
Borbely AA, Wirz-Justice A (1982): Sleep, sleep deprivation and
acetylcholinesterase inhibition by rivastigmine in humans.
depression: A hypothesis derived from a model of sleep
J Clin Psychopharmacol 19:513–521.
regulation. Hum Neurobiol 1:205–210.
Kilduff TS, Peyron C (2000): The hypocretin/orexin ligand-
Chemelli RM, Willie JT, Sinton CM, Elmquist JK, Scammell T,
receptor system: Implications for sleep and sleep disorders.
Lee C, et al (1999): Narcolepsy in orexin knockout mice:
Trends Neurosci 23:359 –365.
Molecular genetics of sleep regulation. Cell 98:437–451.
Kleitman N (1939): Sleep and Wakefulness. Chicago: University
Daniels E, King MA, Smith IE, Shneerson JM (2001): Health-
related quality of life in narcolepsy. J Sleep Res 10:75–81.
Kripke DF, Mullaney DJ, Atkinson MS, Wolf C (1987): Circa-
de Lecea L, Kilduff TS, Peyron C, Gao X, Foye PE, Danielson
dian rhythm disorders in manic-depressives. Biol Psychol
PE, et al (1998): The hypocretins. Hypothalamus-specific
peptides with neuroexcitatory activity. Proc Natl Acad Sci
Kupfer DJ, Ehlers CL, Frank E, Grochocinski VJ, McEachran
AB (1991): EEG sleep profiles and recurrent depression. Biol
Detre TP, Himmelhoch JM, Swartzburg M, Anderson CM, Byck
R, Kupfer DJ (1972): Hypersomnia and manic-depressive
Kuru M, Ueta Y, Serino R, Nakazato M, Yamamoto Y, Shibuya
disease. Am J Psychiatry 128:1303–1305.
I, et al (2000): Centrally administered orexin/hypocretin
Di Chiro G, Hammock MK, Bleyer WA (1976): Spinal descent
activates HPA axis in rats. Neuroreport 11:1977–1980.
of cerebrospinal fluid in man. Neurology 26:1–8.
Lin L, Faraco J, Li R, Kadotani H, Rogers W, Lin X, et al (1999):
Duncan WC, Johnson KA, Sutin E, Wehr TA (1998): Disruption
The sleep disorder canine narcolepsy is caused by a mutation
of the activity-rest cycle by MAOI treatment. Dependence on
in the hypocretin (orexin) receptor 2 gene. Cell 98:365–376.
light and a secondary visual pathway to the circadian pace-
Maes M, Meltzer HY (1995): The serotonin hypothesis of major
maker. Brain Res Bull 45:457–465.
depression. In: Bloom F, Kupfer D, editors. Psychopharma-
Estabrook IV, McCarthy MT, Ko E, Chou TC, Chemelli RM,
cology. The Fourth Generation of Progress. New York:
Yanagisawa M, et al (2001): Fos expression in orexin neurons
varies with behavioral state. J Neurosci 21:1656 –1662.
Marcus JN, Aschkenasi CJ, Lee CE, Chemelli RM, Saper CB,
First MB, Spitzer RL, Gibbon M, Williams JB (1996a): Struc-
Yanagisawa M, et al (2001): Differential expression of orexin
tured Clinical Interview for DSM-IV Axis I Disorders (SCID-
receptors 1 and 2 in the rat brain. J Comp Neurol 435:6 –25. I/P), 2nd ed. New York: Biometrics Research Department,
Mazure C, Nelson JC, Price LH (1986): Reliability and validity
New York State Psychiatric Institute.
of the symptoms of major depressive illness. Arch Gen
First MB, Spitzer RL, Gibbon M, Williams JB, Benjamin L
(1996b): Structured Clinical Interview for DSM-IV Axis II
Mignot E (2001): A commentary on the neurobiology of
Disorders (SCID-II), 2nd ed. New York: Biometrics Research
the hypocretin/orexin system. Neuropsychopharmacology
Department, New York State Psychiatric Institute.
Fujiki N, Yoshida Y, Ripley B, Honda K, Mignot E, Nishino S
Mignot EM, Lammers GJ, Ripley B, Okun M, Nevsimalova S,
(2001): Changes in CSF hypocretin-1 (orexin A) levels in rats
Overeem S, et al (2002): The role of CSF hypocretin
across 24 hours and in response to food deprivation. Neuro-
measurement in the diagnosis of narcolepsy and hypersomnia.
Gillin JC, Buchsbaum M, Wu J, Clark C, Bunney W Jr (2001):
Nishino S, Mao J, Sampathkumaran R, Shelton J, Mignot E
Sleep deprivation as a model experimental antidepressant
(1998): Increased dopaminergic transmission mediates the
treatment: Findings from functional brain imaging. Depress
wake-promoting effects of CNS stimulants. Sleep Res Online
Healy D (1987): Rhythm and blues. Neurochemical, neurophar-
Nishino S, Ripley B, Overeem S, Lammers GJ, Mignot E (2000):
macological and neuropsychological implications of a hy-
Hypocretin (orexin) deficiency in human narcolepsy. Lancet
pothesis of circadian rhythm dysfunction in the affective
disorders. Psychopharmacology 93:271–285.
Nishino S, Ripley B, Overeem S, Nevsimalova S, Lammers GJ,
Holsboer F (2001): Stress, hypercortisolism and corticosteroid
Vankova J, et al (2001): Low cerebrospinal fluid hypocretin
receptors in depression. Implications for therapy. J Affect
(orexin) and altered energy homeostasis in human narcolepsy.
Hungs M, Mignot E (2001): Hypocretin/orexin, sleep and nar-
Nowell PD, Buysse DJ (2001): Treatment of insomnia in patients
colepsy. Bioessays 23:397–408.
with mood disorders. Depress Anxiety 14:7–18.
Janowsky SJ, Overstreet DH (1995): The role of acetylcholine
Peyron C, Faraco J, Rogers W, Ripley B, Overeem S, Charnay Y,
mechanisms in mood disorders. In: Bloom F, Kupfer D,
et al (2000): A mutation in a case of early onset narcolepsy
editors. Psychopharmacology. The Fourth Generation of
and a generalized absence of hypocretin peptides in human
Progress. New York: Raven Press, 945–956.
narcoleptic brains. Nat Med 6:991–997.
Peyron C, Tighe DK, van den Pol AN, de Lecea L, Heller HC,
Van den Hoofdakker RH (1994): Chronobiological theories of
Sutcliffe JG, et al (1998): Neurons containing hypocretin
nonseasonal affective disorders and their implications for
(orexin) project to multiple neuronal systems. J Neurosci
treatment. J Biol Rhythms 9:157–183.
Van den Hoofdakker RH, Beersma DG (1988): On the contri-
Reynolds CF, Gillin JC, Kupfer DJ (1987): Sleep and affective
bution of sleep wake physiology to the explanation and the
disorders. In: HY Meltzer, editor. Psychopharmacology: The
treatment of depression. Acta Psychiatr Scand Suppl 341:53–
Third Generation of Progress. New York: Raven Press, 647–
van den Pol AN (1999): Hypothalamic hypocretin (orexin).
Ringel BL, Szuba MP (2001): Potential mechanisms of the sleep
Robust innervation of the spinal cord. J Neurosci 19:3171–
therapies for depression. Depress Anxiety 14:29 –36.
Ripley B, Overeem S, Fujiki N, Nevsimalova S, Uchino M,
Yesavage J, et al (2001): CSF hypocretin/orexin levels in
Willie JT, Chemelli RM, Sinton CM, Yanagisawa M (2001): To
narcolepsy and other neurological conditions. Neurology
eat or to sleep? Orexin in the regulation of feeding and
wakefulness. Annu Rev Neurosci 24:429 –458.
Russell SH, Small CJ, Dakin CL, Abbott CR, Morgan DG,
Willner P (1995): Dopaminergic mechanisms in depression. In:
Ghatei MA, et al (2001): The central effects of orexin-A in
Bloom F, Kupfer D, editors. Psychopharmacology. The
the hypothalamic-pituitary-adrenal axis in vivo and in vitro in
Fourth Generation of Progress. New York: Raven Press,
male rats. J Neuroendocrinol 13:561–566.
Sakurai T, Amemiya A, Ishii M, Matsuzaki I, Chemelli RM,
Winokur A, Gary KA, Rodner S, Rae-Red C, Fernando AT,
Tanaka H, et al (1998): Orexins and orexin receptors: A
Szuba MP (2001): Depression, sleep physiology, and antide-
family of hypothalamic neuropeptides and G protein-coupled
pressant drugs. Depress Anxiety 14:19 –28.
receptors that regulate feeding behavior. Cell 92:573–585.
Wirz-Justice A (1995): Biological rhythms in mood disorders. In:
Sakurai T, Moriguchi T, Furuya K, Kajiwara N, Nakamura T,
Bloom F, Kupfer D, editors. Psychopharmacology. The
Yanagisawa M, et al (1999): Structure and function of human
Fourth Generation of Progress. New York: Raven Press,
prepro-orexin gene. J Biol Chem 274:17771–17776.
Schatzberg A, Schildkraut JJ (1995): Recent studies on norepi-
Wu JC, Bunney WE (1990): The biological basis of an antide-
nephrine systems in mood disorders. In: Bloom F, Kupfer D,
pressant response to sleep deprivation and relapse. Review
editors. Psychopharmacology. The Fourth Generation ofProgress. New York: Raven Press, 911–920.
and hypothesis. Am J Psychiatry 147:14 –21.
Shelton RC, Winn S, Ekhatore N, Loosen PT (1993): The effects
Yoshida Y, Fujiki N, Nakajima T, Ripley B, Matsumura H,
of antidepressants on the thyroid axis in depression. Biol
Yoneda H, et al (2001): Fluctuation of extracellular hypocre-
tin-1 (orexin A) levels in the rat in relation to the light-darkcycle and sleep-wake activities. Eur J Neurosci 14:1075–
Steiner M, Werstiuk ES, Seggie J (1987): Dysregulation of
neuroendocrine crossroads: Depression, circadian rhythmsand the retina—a hypothesis. Prog Neuropsychopharmacol
Young EA, Haskett RF, Murphy-Weinberg V, Watson SJ, Akil
Biol Psychiatry 11:267–278.
H (1991): Loss of glucocorticoid fast feedback in depression.
Taheri S, Zeitzer JM, Mignot E (2002): The role of hypocretins
Arch Gen Psychiatry 48:693–699.
(orexins) in sleep regulation and narcolepsy. Ann Rev Neu-
Zeitzer JM, Buckmaster CL, Parker KJ, Hauck CM, Lyons DM,
Mignot E (2002): Diurnal variation of hypocretin-1 in the
Thannickal TC, Moore RY, Nienhuis R, Ramanathan L, Gulyani
cisternal cerebrospinal fluid of a diurnal sleep-consolidating
S, Aldrich M, et al (2000): Reduced number of hypocretin
primate, Saimiri sciureus. Soc Res Biol Rhythms 8th Annual
neurons in human narcolepsy. Neuron 27:469 –474.
A SMOKE-FREE ZONE with NLP One year on since the smoking ban, T he ban on smoking in public places your health, plus public opinion granting Many smokers have mixed feelings about it honorary pariah status, combined with quitting: they want to lose the disadvantages the current legislation making it so darned of smoking but don’t want to lose the benefits. polls, ‘three quarters of
Patient Information Surname_________________________________ First Name __________________________ Initial__________ Date of Birth (DD/MM/YYYY) ______________________ Sex M □ F □ Address ____________________________________________________________________ Apt # __________ City __________________________________ Province ____________________ Postal Code _______________ Home Phone#
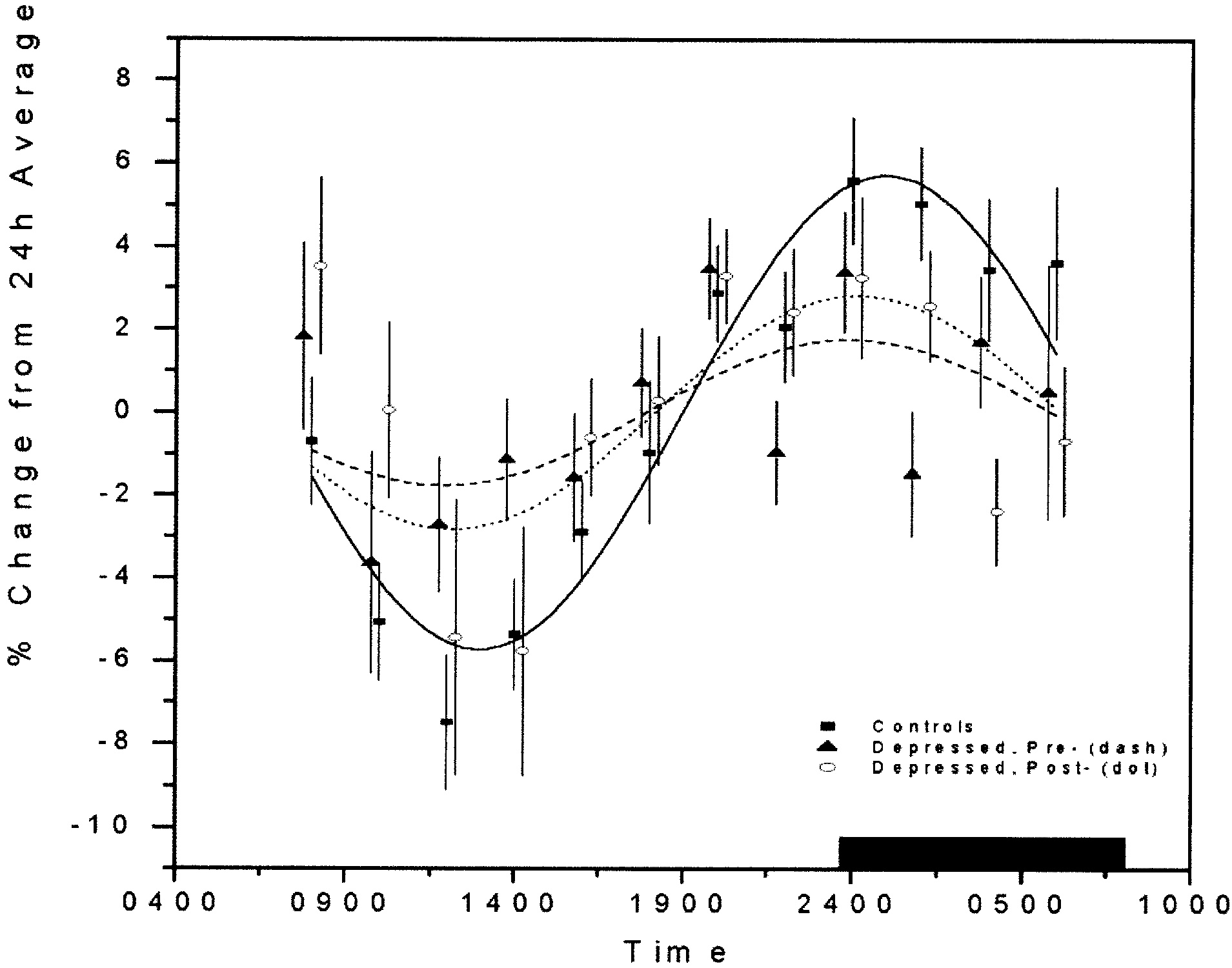 Table 2. Sinusoidal Curve Fitting in Control and Depressed Subjects
Data are mean Ϯ SD. Times are given as 24-hour clock times.
Table 2. Sinusoidal Curve Fitting in Control and Depressed Subjects
Data are mean Ϯ SD. Times are given as 24-hour clock times.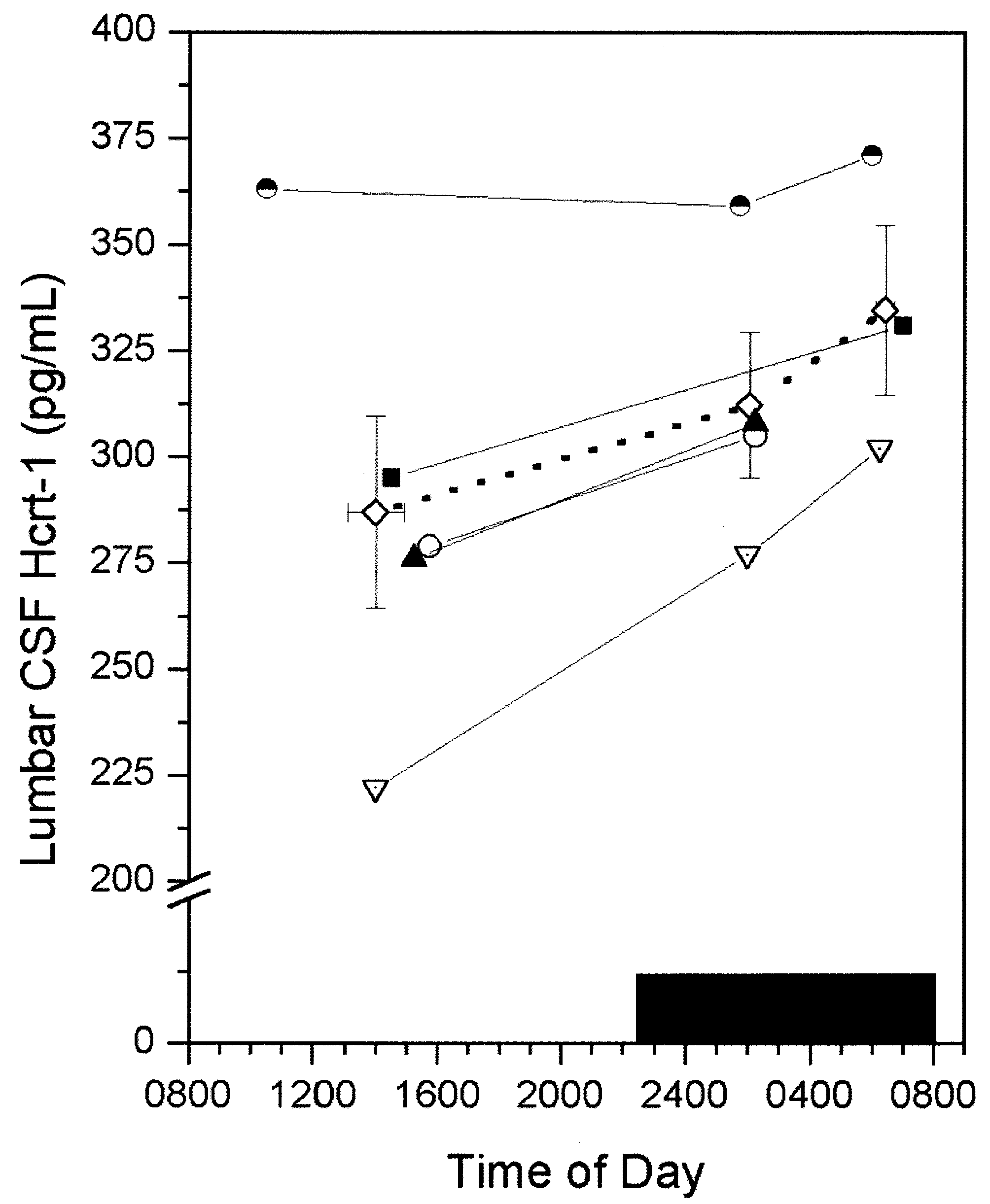 Basal Levels of Hypocretin-1 in Depressed andControl Subjects
Basal 24-hour, daytime, and nighttime levels did not differbetween supine control subjects and untreated patients, butslightly higher levels were observed in depressed subjects,especially during the day (daytime concentrations in con-trol subjects 251.7 Ϯ 11.5 pg/mL and in pretreatmentdepressed subjects 275.8 Ϯ 11.5 pg/mL, nighttime con-centrations in control subjects 274.0 Ϯ 10.6 pg/mL and inpretreatment depressed 280.9 Ϯ 12.2 pg/mL, mean-24hour concentrations in control subjects 265.0 Ϯ 11.0pg/mL and in pretreatment depressed subjects 281.2 Ϯ11.8 pg/mL, differences not significant; Thesevalues were also similar to previously reported data inambulatory control subjects and markedly higher thanlevels observed in narcolepsy. As suspected from thesinusoid analysis, there was a highly significant differencebetween daytime (11:00 AM– 6:00 PM) and night time(11:00 PM– 6:00 AM) hypocretin-1 concentrations in con-trol subjects (p Ͻ .001, paired two-tailed t test). Theday-night difference was lost in depressive subjects before(p ϭ .32, paired two-tailed t test) or after (p ϭ .24, pairedtwo-tailed t test) treatment.
Basal Levels of Hypocretin-1 in Depressed andControl Subjects
Basal 24-hour, daytime, and nighttime levels did not differbetween supine control subjects and untreated patients, butslightly higher levels were observed in depressed subjects,especially during the day (daytime concentrations in con-trol subjects 251.7 Ϯ 11.5 pg/mL and in pretreatmentdepressed subjects 275.8 Ϯ 11.5 pg/mL, nighttime con-centrations in control subjects 274.0 Ϯ 10.6 pg/mL and inpretreatment depressed 280.9 Ϯ 12.2 pg/mL, mean-24hour concentrations in control subjects 265.0 Ϯ 11.0pg/mL and in pretreatment depressed subjects 281.2 Ϯ11.8 pg/mL, differences not significant; Thesevalues were also similar to previously reported data inambulatory control subjects and markedly higher thanlevels observed in narcolepsy. As suspected from thesinusoid analysis, there was a highly significant differencebetween daytime (11:00 AM– 6:00 PM) and night time(11:00 PM– 6:00 AM) hypocretin-1 concentrations in con-trol subjects (p Ͻ .001, paired two-tailed t test). Theday-night difference was lost in depressive subjects before(p ϭ .32, paired two-tailed t test) or after (p ϭ .24, pairedtwo-tailed t test) treatment.