C l i n i c a l C a r e / E d u c a t i o n / N u t r i t i o n O R I G I N A L The Synergistic Effect of Miglitol Plus Metformin Combination Therapy in the Treatment of Type 2 Diabetes EAN-LOUIS CHIASSON, MD ISA NADITCH, MD FOR THE MIGLITOL CANADIAN UNIVERSITY
mode of action; it blocks oligosaccharide
INVESTIGATOR GROUP
catabolism, delays carbohydrate diges-tion and absorption, and smooths andlowers postprandial plasma blood glu-cose peaks (6 –9). Substantial evidencesupports their use as monotherapy or ad-
OBJECTIVE — To investigate the efficacy and safety of miglitol in combination with met-
junct therapy for poorly controlled type 2
formin in improving glycemic control in outpatients in whom type 2 diabetes is insufficiently
diabetes (5,10 –14). Miglitol is the first
RESEARCH DESIGN AND METHODS — In this multicenter, double-blind, placebo-
controlled study, 324 patients with type 2 diabetes were randomized, after an 8-week placebo
run-in period, to treatment with either placebo, miglitol alone, metformin alone, or miglitol plus
metformin for 36 weeks. The miglitol was titrated to 100 mg three times a day and metformin was
administered at 500 mg three times a day. The primary efficacy criterion was change in HbA1c
nylureas (11) as a glucose-lowering agent
from baseline to the end of treatment. Secondary parameters included changes in fasting and
postprandial plasma glucose and insulin levels, serum triglyceride levels, and responder rate.
number of clinical studies. A study ofmiglitol in combination with metformin
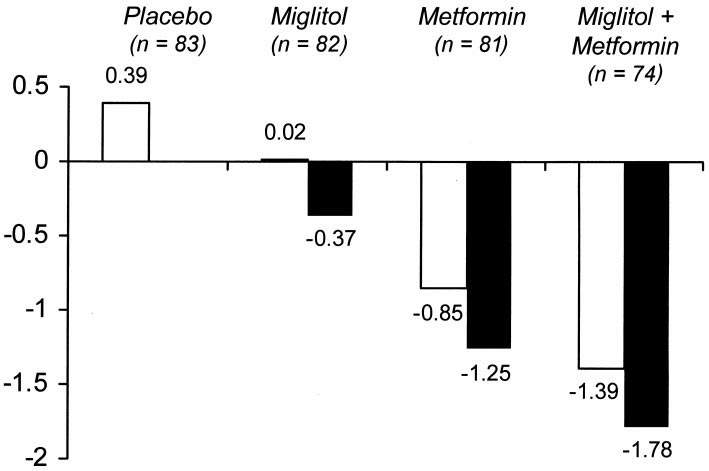
RESULTS — A total of 318 patients were valid for intent-to-treat analysis. A reduction in mean
of Ϫ1.78% was observed with miglitol plus metformin combination
therapy, which was significantly different from treatment with metformin alone (Ϫ1.25; P ϭ
type 2 diabetic patients (18). However, it
0.002). Miglitol plus metformin also resulted in better metabolic control than metformin alone
is still unclear whether miglitol can en-
for fasting plasma glucose (Ϫ44.8 vs. Ϫ20.4 mg/dl; P ϭ 0.0025), 2-h postprandial glucose area
under the curve (Ϫ59.0 vs. –18.0 mg/dl; P ϭ 0.0001), and responder rate (70.6 vs. 45.52%; P ϭ
0.0014). All therapies were well tolerated.
aged type 2 diabetic patients and whetherthe safety and tolerability profile of migli-
CONCLUSIONS — In type 2 diabetic patients, miglitol in combination with metformin
gives greater glycemic improvement than metformin monotherapy.
fected by such a combination. Therefore,this study was performed to investigate
Diabetes Care 24:989 –994, 2001
the efficacy and safety of miglitol in com-bination with metformin in improvingglycemic control, compared with met-
Maintainingnormalplasmaglucose in combination. The biguanide met- formin monotherapy, in middle-aged
formin is a frequent first-line choice of
insufficiently controlled by diet alone.
dations supported by recent data from the
agent eventually necessitates the use of in-
exercise as the first-line approach, fol-
atic -cell function (5) and eventually re-
RESEARCH DESIGN AND
antihyperglycemic agents, either alone or
METHODS — This was a multicenter,
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Research Group on Diabetes and Metabolic Regulation, Research Center, Centre Hospitalier de
controlled parallel group study. Eligible
l’Universite´ de Montre´al, Montreal, Quebec, Canada; and 2Sanofi-Synthelabo, Paris, France.
Address correspondence and reprint requests to Jean-Louis Chiasson, MD, Research Group on Diabetes
and Metabolic Regulation, Research Center CHUM, Hoˆtel-Dieu CHUM, 3850 St. Urbain, 8 –202, Montreal,Quebec, Canada H2W 1T8. E-mail: [email protected].
Received for publication 28 November 2000 and accepted in revised form 6 February 2001.
L.N. is an employee of Sanofi-Synthelabo, which is involved in the marketing of the product miglitol for
Abbreviations: AUC, area under the curve; ITT, intent to treat. A table elsewhere in this issue shows conventional and Syste`me International (SI) units and conversion
DIABETES CARE, VOLUME 24, NUMBER 6, JUNE 2001
Miglitol plus metformin in type 2 diabetes
events, gastrointestinal diseases, medica-
tions likely to affect intestinal motility or
meal. The proportion of responders in the
different treatment groups was also eval-
tivity to miglitol or metformin, and a his-
uated, in which a clinically significant re-
tory of lactic acidosis. Patients who were
analysis of variance techniques. All four
ing, at week –2 and baseline, and there-
procedures, patients who fulfilled the el-
igibility criteria gave their written in-
20, 28, and 36) after randomization. Rou-
sured at week Ϫ2 and at every subsequent
least one dose of trial medication were in-
diet (19). They were also advised regard-
ing exercise, mainly walking 20 –30 min
at least three times per week. The diet was
analyzed in terms of the percentage of pa-
reinforced after 1 month, and if the HbA1c
gated by the occurrence of adverse events;
considered dietary failure. Patients with
RESULTS — A total of 324 patients
were eligible for randomization to match-
transketolase, folate, vitamin B12, vitamin
A, and retinol protein binding), and stan-
and at all visits thereafter. Routine bio-
force-titrated as follows: administration
values after randomization. A total of 318
formed at baseline and at the final visit.
ters and clinical data for all randomized
tal signs and weight were recorded at each
patients, age, race (predominately Cauca-
sian), weight and BMI, sex ratio, duration
200.3 Ϯ 93.3 days; miglitol 190.9 Ϯ 90.5
were performed at a central laboratory.
change in HbA1c level from baseline to the
end of the double-blind treatment for the
To detect a mean difference of 0.6% in the
groups from baseline to the end of treat-
ment, with ␣ ϭ 0.05 and a power (1–) of
per treatment group were required. To ac-
prandial plasma glucose and insulin levels
count for multicenter variability, this was
different treatments are shown in Table 2.
increased by 20% to 75 patients per treat-
There was an increase of 0.38 Ϯ 0.12% in
line to the end of treatment, measured at
the placebo group, virtually no change in
the miglitol group (0.02 Ϯ 0.10%), a de-
formin group, and a decrease of Ϫ1.39 Ϯ
DIABETES CARE, VOLUME 24, NUMBER 6, JUNE 2001
Chiasson and Naditch Table 1—Demographic and clinical data on randomized patients
compared with metformin monotherapy(34.6%).
active treatment groups, in contrast to an
increase in patients taking placebo (Table
therapy were significantly greater (P Ͻ
fasting plasma glucose was also greater in
receiving metformin monotherapy (P ϭ
prandial plasma insulin at 60 min did not
reach statistical significance for the com-
Data are means Ϯ SD and n (%). MIG, miglitol; MET, metformin.
monotherapy, a statistically significantdifference was observed in favor of the
combination group (P ϭ 0.002, compar-
(P ϭ 0.0143 and 0.0177, respectively)
actual treatment effect is illustrated in Fig.
(P ϭ 0.0014) more patients were classi-
fied as responders (i.e., showed Ն15% re-
pared with placebo was – 0.37% for migli-
tients’ disease status. Because the patients
which stimulates release of pancreatic in-
sulin. It is clear that lower postprandial
plasma insulin levels despite higher post-
Table 2—Mean change from baseline in selected study variables (ITT population)
Incremental plasma glucose AUC (mg ⅐ h/dl)
Incremental plasma insulin AUC (pmol ⅐ h/l)
Data are mean Ϯ SE. NS, not significant, MIG, miglitol, MET, metformin.
DIABETES CARE, VOLUME 24, NUMBER 6, JUNE 2001
Miglitol plus metformin in type 2 diabetes
and 19 (25.0%) in the metformin plusmiglitol combination therapy group. Flat-ulence and diarrhea were the most com-mon adverse events associated withpremature discontinuation from the study.
rious adverse events postrandomization:3 of these events occurred in the placebogroup, 2 in the miglitol group, 4 in themetformin group, and 9 in the metforminplus miglitol combination group. None ofthese serious adverse events were deemedby the investigators to be either probablyor possibly related to the study drug. Nodeaths occurred during this study. No se-vere hypoglycemic episodes were re-ported. The rate of hypoglycemia wasslightly higher in patients receiving met-formin plus miglitol combination therapy(13.2 vs. 9.6% receiving metformin), butthis difference was not clinically significant.
Figure 1—The mean absolute change (open bar) and the placebo-subtracted change (closed bar)in HbA from baseline to end of treatment for miglitol monotherapy, metformin monotherapy, and
clinically or statistically significant differ-
miglitol plus metformin combination therapy.
ences in hematological and biochemicalparameters or urinalysis. One patient inthe metformin group showed an elevation
decreased -cell function. This could be
caused by glucotoxicity resulting from in-
alanine aminotransferase, but this was not
which is an increased incidence of 3.4%.
considered clinically relevant. Glycosuria
from baseline to the end of treatment did
gastrointestinal; flatulence and diarrhea
laboratory abnormality or change in vital
signs during the study. Although all treat-
those receiving the other treatments.
the safety analysis. After randomization,
tients discontinued the study prematurely
because of adverse events: 2 (2.4%) in the
placebo group, 11 (13.4%) in the miglitol
the other treatment groups: Ϫ1.87 kg formetformin plus miglitol combination
Table 3—Incidence of most common adverse events
compared with – 0.79 kg for metforminalone, – 0.42 kg for miglitol alone, and
Ϫ0.69 kg for placebo (P ϭ NS). CONCLUSIONS — Previous studies
tion with sulfonylureas in type 2 diabetes
tic effect on glycemic control, as indicated
Data are n (%). Common adverse events are considered those with incidence
patients in whom type 2 diabetes is insuf-
group. MIG, miglitol, MET, metformin.
DIABETES CARE, VOLUME 24, NUMBER 6, JUNE 2001
Chiasson and Naditch
ication. It is possible that slower titration
significantly greater reductions in HbA1c,
rectly by increasing peripheral tissue sen-
of miglitol would reduce the gastrointes-
sitivity to insulin (27); miglitol acts at the
tinal side effects and improve compliance,
small intestine by delaying the digestion
resulting in better improvement in HbA1c.
the end of treatment of patients receiving
formin was found to be safe and well tol-
erated in the study cohort. The incidence
given by current clinical practice recom-
decreasing insulin resistance (29), which
mechanism of action of an ␣-glucosidase
inhibitor. It is possible that slower titra-
tributory factor to the superiority of the
tion of the drug, as with acarbose, could
diminish the incidence of gastrointestinal
side effects (32). Overall, the incidence of
did not have any significant effect on fast-
side effects with metformin plus miglitol
cally significant in achieving the treat-
ment goal. The clinical importance of this
formin alone (Ϫ12.4 Ϯ 3.8 vs. Ϫ17.4 Ϯ
cantly different from that observed for ei-
4.7 pmol/l; P ϭ NS), it did have a ten-
abetes Study data, which indicates that for
dency to decrease the postprandial incre-
although the rate of discontinuations was
trend toward an increase in the number of
complications (24). The superiority of the
17.7 pmol ⅐ h/l; P ϭ 0.059). This is prob-
gastrointestinal side effects in the met-
ably caused by the effect of miglitol be-
strated by the higher response rate of pa-
cause miglitol alone resulted in a decrease
dence of any serious adverse events asso-
Ϫ72.8 Ϯ 21.9 pmol ⅐ h/l. The reduction ciated with this combination regimen. No
those of Mooradian in elderly type 2 dia-
lin could result in improved insulin sen-
served in this study, and the incidence of
sitivity, as we have shown in elderly type
ments. The lack of deleterious effects on
macrovascular complications (25,26).
liver enzymes indicates that regular mon-
sulted in a treatment effect of Ϫ0.37% in
itoring of liver function during combina-
dial plasma glucose peaks in clinical prac-
HbA1c compared with placebo (Fig. 1).
plasma glucose levels. Because ␣-glucosi-
(11,13,22,23,31), in which a reduction in
dase inhibitors have been reported previ-
monosaccharide ␣-glucosidase inhibitor,
shown. It is interesting that Johnston et al.
plasma glucose peaks (8 –10), miglitol in
(11) could not show any better efficacy of
formin alone, with a good safety profile,
as well as overall glycemic control, espe-
cially for patients with postprandial hyper-
the test meal. It is possible that the discor-
insufficiently controlled by diet alone.
glycemia refractory to other treatments.
tically to confer this additional glycemic
because of increased gastrointestinal side
effects. Similarly, in the present study, the
and macrovascular diabetic complications.
gested that the administration of the two
drugs together has a synergistic effect on
with metformin alone (Ϫ34.7 Ϯ 7.2 vs. Acknowledgments — This study was funded
glycemic control; this is plausible because
Ϫ18.0 Ϯ 7.3 mg ⅐ h/dl; P Ͻ 0.001), con- by an unrestricted research grant from Bayer
firming the efficacy of the drug. Again, the
Canada, Inc., and additional financial support
glucose levels through completely differ-
was received from Sanofi-Synthelabo.
We thank the coordinating nurses and die-
on the liver directly by decreasing hepatic
ticians in all centers for their contribution.
DIABETES CARE, VOLUME 24, NUMBER 6, JUNE 2001
Miglitol plus metformin in type 2 diabetes
This study was presented as a poster at the
emergence of ␣-glucosidase inhibitors.
60th annual scientific sessions of the American
21. Rossetti L, Giaccari A, DeFronzo RA: Glu-
Diabetes Association, San Antonio, Texas,
9. Holman RR, Steemson J, Turner RC: Post-
cose toxicity. Diabetes Care 13:610 – 630,
prandial glycaemic reduction by an ␣-glu-
cosidase inhibitor in type 2 diabetic patients
22. Johnston PS, Feig PU, Coniff RF, Krol A,
APPENDIX
with therapeutically attained basal normo-
glycaemia. Diabetes Res 18:149 –153, 1991
The Miglitol University Canadian Investi-
10. Heinz G, Komjati M, Korn A, Waldhausl
patients with ␣-glucosidase inhibition.
gator Group included: Dr. Hertzel C. Ger-
Diabetes Care 21:416 – 422, 1998
23. Johnston PS, Feig PU, Coniff RF, Krol A,
Center; Dr. Robert J. Josse, St. Michael’s
Miglitol (BAY m 1099) in type II diabetes. Eur J Clin Pharmacol 37:33–36, 1989
trated-dose ␣-glucosidase inhibition in
Hospital; Dr. Lawrence A. Leiter, St. Mi-
Santiago JV, Pi-Sunyer FX, Krol A: Effects
patients. Diabetes Care 21:409 – 415, 1998
Dr. N. Wilson Rodger, St. Joseph’s Health
of the carbohydrase inhibitor miglitol in
24. Stratton IM, Adler AI, Neil HA, Matthews
sulfonylurea-treated NIDDM patients. Di-
versity of Toronto, Toronto, ON; Dr. John
A. Hunt, Lion’s Gate Hospital; Dr. Hugh
vascular complications of type 2 diabetes
Maheux, Center Universitaire de Sante´ de
l’Estrie; Dr. Jean-Franc¸ois Yale, McGill
25. Hanefeld M, Fischer S, Julius U, Schulze J,
13. Segal P, Feig PU, Schernthaner G, Ratz-
Risk factors for myocardial infarction and
The efficacy and safety of miglitol therapy
low-up. Diabetologia 39:1577–1583, 1996
26. Coutinho M, Gerstein HC, Wang Y, Yusuf
diet alone. Diabetes Care 20:687– 691,
14. Escobar-Jimenez F, Barajas C, De Leiva A,
egression analysis of published data from
20 studies of 95,783 individuals followed
References
Hernandez-Mijares A, Pinon F, de la Calle
for 12.4 years. Diabetes Care 22:233–240,
1. U.K. Prospective Diabetes Study Group:
H, Tebar J, Soler J, Cobos A, Guardiola E,
Intensive blood-glucose control with sul-
and the Miglitol Collaborative Group: Ef-
27. Inzucchi SE, Maggs DG, Spollett GR, Page
ficacy and tolerability of miglitol in the
plications in patients with type 2 diabetes
dependent diabetes mellitus. Curr Ther
(UKPDS 33). Lancet 352:837– 853, 1998
and troglitazone in type II diabetes melli-
2. U.K. Prospective Diabetes Study Group:
15. Saunier B, Kilker RD Jr, Tkacz JS, Quaroni
tus. N Engl J Med 338:867– 872, 1998
Effect of intensive blood-glucose control
field JE: Regulation of the absorption of
weight patients with type 2 diabetes (UK-
PDS 34). Lancet 352:854 – 865, 1998
cessing glucosidases. J Biol Chem 257:
glucosidase inhibitors. Gut 27:1471–
16. Scott LJ, Spencer CM: Miglitol: a review of
its therapeutic potential in type 2 diabetes
Meier A, Thaete FL: Effects of weight loss
non-insulin-dependent diabetes mellitus.
mellitus. Drugs 59:521–549, 2000
17. Pagano G, Marena S, Corgiat-Mansin L,
sensitivity in obesity. Diabetes 48:839 –
4. Johansen K: Efficacy of metformin in the
treatment of NIDDM: meta-analysis. Dia-
clamide in diet-treated type 2 diabetic pa-
tients. Diabete Metab 21:162–167, 1995
Acarbose: its role in the treatment of dia-
18. Mooradian AD: Drug therapy of non-in-
betes mellitus. Ann Pharmacother 30:
acarbose on insulin sensitivity in elderly
patients with diabetes. Diabetes Care 23:
6. Bischoff H: Pharmacology of ␣-glucosi-
19. Franz MJ, Horton ES, Bantle JP, Beebe
dase inhibition. Eur J Clin Invest 24
31. Lebovitz HE: ␣-glucosidase inhibitors as
agents in the treatment of diabetes. Diabe-
principles for the management of diabetes
The effect of miglitol and acarbose after an
and related complications. Diabetes Care
32. May C: Efficacy and tolerability of step-
mechanism? Br J Clin Pharmacol 30:391–
dards of medical care for patients with di-
8. Lebovitz HE: Oral antidiabetic agents: the
abetes mellitus. Diabetes Care 22 (Suppl.
reas. Diabetes Und Stoffwechsel 4:3– 8, 1995
DIABETES CARE, VOLUME 24, NUMBER 6, JUNE 2001
ECONOMIC SECURITY CORP. OF SW AREA/WOMEN’S HEALTH CARE 302 JOPLIN, JOPLIN, MO 64801 PHONE 417-781-4788 REQUEST FOR TREATMENT AND PRESCRIPTION OR INSERTION OF CONTRACEPTIVE DRUG, DEVICE OR METHOD. I hereby request that a person authorized by Economic Security Corporations Women’s Health Care & Family Planning program examine and treat me and that a suitable contraceptive drug, device or m
Using synergies – How active agents and cream published in Kosmetische Praxis 2010 (3), 10-12 No doubt – the grey area between pharmaceutical and cosmetic skin care products is expanding. Dermaceuticals and dermocosmetics are keywords which demonstrate that the cosmetic product market is gaining grounds in the pharmaceutical field, not least because of legal claims for a proof of efficiency.
 Miglitol plus metformin in type 2 diabetes
Miglitol plus metformin in type 2 diabetes