Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Lpc flow at 3/6/04
LOCAL PRODUCT CIRCULAR LPC-EMD-C-122002a-Malaysia
There are no clinical data in patients with severe hepatic insufficiency (Child-Pugh score >9). Capsules V. CLINICAL STUDIES Oral administration of EMEND in combination with ondansetron and dexamethasone (aprepitant regimen) has been
shown to prevent acute and delayed nausea and vomiting associated with highly emetogenic chemotherapy including
I. THERAPEUTIC CLASS
In 2 multicenter, randomized, parallel, double-blind, controlled clinical studies, the aprepitant regimen (see table below)
EMEND® (aprepitant, MSD), is a substance P neurokinin 1 (NK1) receptor antagonist.
was compared with standard therapy in patients receiving a chemotherapy regimen that included cisplatin >50 mg/m2
II. CLINICAL PHARMACOLOGY
(mean cisplatin dose = 80.2 mg/m2). Of the 550 patients who were randomized to receive the aprepitant regimen, 42%
were women, 58% men, 59% White, 3% Asian, 5% Black, 12% Hispanic American, and 21% Multi-Racial. The aprepitant-
Aprepitant has a unique mode of action; it is a selective high affinity antagonist at human substance P neurokinin 1 (NK
treated patients in these clinical studies ranged from 14 to 84 years of age, with a mean age of 56 years. 170 patients
receptors. Counter-screening assays showed that aprepitant was at least 3,000-fold selective for the NK
were 65 years or older, with 29 patients being 75 years or older.
other enzyme, transporter, ion channel and receptor sites including the dopamine and serotonin receptors that are
Patients (N = 1105) were randomized to either the Aprepitant Regimen (N = 550) or standard therapy (N = 555). The
targets for existing Chemotherapy-Induced Nausea and Vomiting (CINV) therapies.
treatment regimens are defined in the table below.
NK1-receptor antagonists have been shown pre-clinically to inhibit emesis induced by cytotoxic chemotherapeutic agents,
Treatment Regimens
such as cisplatin, via central actions. Preclinical and human Positron Emission Tomography (PET) studies with aprepitant
have shown that it is brain penetrant and occupies brain NK1 receptors. Preclinical studies show that aprepitant has a
Aprepitant 80 mg PO Daily (Days 2 and 3 only)
long duration of central activity, inhibits both the acute and delayed phases of cisplatin-induced emesis, and augments
the antiemetic activity of the 5-HT3-receptor antagonist ondansetron and the corticosteroid dexamethasone against
IIb-1. AbsorptionThe mean absolute oral bioavailability of aprepitant is approximately 60 to 65% and the mean peak plasma concentration(Cmax) of aprepitant occurred at approximately 4 hours (Tmax). Oral administration of the capsule with a standard breakfast
Aprepitant placebo and dexamethasone placebo were used to maintain blinding.
had no clinically meaningful effect on the bioavailability of aprepitant.
During these studies 95% of the patients in the aprepitant group received a concomitant chemotherapeutic agent in
The pharmacokinetics of aprepitant are non-linear across the clinical dose range. In healthy young adults, the increase in
addition to protocol-mandated cisplatin. The most common chemotherapeutic agents and the number of aprepitant
AUC0-∞ was 26% greater than dose proportional between 80-mg and 125-mg single doses administered in the fed state.
patients exposed follows: etoposide (106), fluorouracil (100), gemcitabine (89), vinorelbine (82), paclitaxel (52),cyclophosphamide (50), doxorubicin (38), docetaxel (11).
Following oral administration of a single 125-mg dose of EMEND on Day 1 and 80 mg once daily on Days 2 and 3, theAUC0-24hr was approximately 19.5 mcg•hr/mL and 20.1 mcg•hr/mL on Day 1 and Day 3, respectively. The Cmax of 1.5 mcg/
The antiemetic activity of EMEND was evaluated during the acute phase (0 to 24 hours post-cisplatin treatment), the
mL and 1.4 mcg/mL were reached in approximately 4 hours (Tmax) on Day 1 and Day 3, respectively.
delayed phase (25 to 120 hours post-cisplatin treatment) and overall (0 to 120 hours post-cisplatin treatment) in Cycle 1. Efficacy was based on evaluation of the following endpoints:
Aprepitant is greater than 95% bound to plasma proteins. The geometric mean apparent volume of distribution at steady
• complete response (defined as no emetic episodes and no use of rescue therapy)
state (Vdss) is approximately 66 L in humans.
Other prespecified (secondary and exploratory) endpoints:
Aprepitant crosses the placenta in rats, and crosses the blood brain barrier in rats and ferrets. PET studies in humans
• complete protection (defined as no emetic episodes, no use of rescue therapy, and a maximum nausea visual analogue
indicate that aprepitant crosses the blood brain barrier (see CLINICAL PHARMACOLOGY, Mechanism of Action).
scale [VAS] score <25 mm on a 0 to 100 mm scale)
• no emesis (defined as no emetic episodes regardless of use of rescue therapy)
Aprepitant undergoes extensive metabolism. In healthy young adults, aprepitant accounts for approximately 24% of the
• no nausea (maximum VAS <5 mm on a 0 to 100 mm scale)
radioactivity in plasma over 72 hours following a single oral 300-mg dose of [14C]-aprepitant, indicating a substantial presence
• no significant nausea (maximum VAS <25 mm on a 0 to 100 mm scale)
of metabolites in the plasma. Seven metabolites of aprepitant, which are only weakly active, have been identified in human
A summary of the key study results from each individual study analysis is shown in Table 1 and Table 2.
plasma. The metabolism of aprepitant occurs largely via oxidation at the morpholine ring and its side chains. In vitro
Table 1 : Percent of Patients Responding by Treatment Group and Phase for Study 1 — Cycle 1
studies using human liver microsomes indicate that aprepitant is metabolized primarily by CYP3A4 with minor metabolismby CYP1A2 and CYP2C19, and no metabolism by CYP2D6, CYP2C9, or CYP2E1.
Aprepitant is eliminated primarily by metabolism; aprepitant is not renally excreted. Following administration of a singleoral 300-mg dose of [14C]-aprepitant to healthy subjects, 5% of the radioactivity was recovered in urine and 86% in feces. PRIMARY ENDPOINT
The apparent plasma clearance of aprepitant ranged from approximately 60 to 84 mL/min. The apparent terminal half-
Complete Response
life ranged from approximately 9 to 13 hours. OTHER PRESPECIFIED (SECONDARY AND EXPLORATORY) ENDPOINTS
Following oral administration of a single 125-mg dose of EMEND, the Cmax for aprepitant is 16% higher in females as
Complete Response
compared with males. The half-life of aprepitant is 25% lower in females as compared with males and its T
approximately the same time. These differences are not considered clinically meaningful. No dosage adjustment for
Complete Protection
ElderlyFollowing oral administration of a single 125-mg dose of EMEND on Day 1 and 80 mg once daily on Days 2 through 5, the
AUC0-24hr of aprepitant was 21% higher on Day 1 and 36% higher on Day 5 in elderly (≥65 years) relative to younger adults.
The Cmax was 10% higher on Day 1 and 24% higher on Day 5 in elderly relative to younger adults. These differences are not
considered clinically meaningful. No dosage adjustment for EMEND is necessary in elderly patients. No Emesis
The pharmacokinetics of EMEND have not been evaluated in patients below 18 years of age.
Following oral administration of a single 125-mg dose of EMEND, the AUC0-24hr is approximately 25% and 29% higher in
No Nausea
Hispanics as compared with Caucasians and Blacks, respectively. The Cmax is 22% and 31% higher in Hispanics ascompared with Caucasians and Blacks, respectively. These differences are not considered clinically meaningful. No
dosage adjustment for EMEND is necessary based on race. No Significant Nausea
EMEND was well tolerated in patients with mild to moderate hepatic insufficiency. Following administration of a single
125-mg dose of EMEND on Day 1 and 80 mg once daily on Days 2 and 3 to patients with mild hepatic insufficiency
(Child-Pugh score 5 to 6), the AUC0-24hr of aprepitant was 11% lower on Day 1 and 36% lower on Day 3, as comparedwith healthy subjects given the same regimen. In patients with moderate hepatic insufficiency (Child-Pugh score 7 to 9),
N: Number of patients (older than 18 years of age) who received cisplatin, study drug, and had at least one post
the AUC0-24hr of aprepitant was 10% higher on Day 1 and 18% higher on Day 3, as compared with healthy subjects given
the same regimen. These differences in AUC
0-24hr are not considered clinically meaningful; therefore, no dosage adjustment
Overall: 0 to 120 hours post-cisplatin treatment.
for EMEND is necessary in patients with mild to moderate hepatic insufficiency.
Acute phase: 0 to 24 hours post-cisplatin treatment.
Delayed phase: 25 to 120 hours post-cisplatin treatment.
There are no clinical or pharmacokinetic data in patients with severe hepatic insufficiency (Child-Pugh score >9).
Visual analogue scale (VAS) score range: 0 mm = no nausea; 100 mm = nausea as bad as it could be.
Table 1 includes nominal p-values not adjusted for multiplicity.
A single 240-mg dose of EMEND was administered to patients with severe renal insufficiency (CrCl<30 mL/min) and topatients with end stage renal disease (ESRD) requiring hemodialysis. Table 2 : Percent of Patients Responding by Treatment Group and Phase for Study 2 — Cycle 1
In patients with severe renal insufficiency, the AUC0-∞ of total aprepitant (unbound and protein bound) decreased by 21%
Aprepitant Regimen Standard Therapy p-Value
max decreased by 32%, relative to healthy subjects. In patients with ESRD undergoing hemodialysis, the AUC0-∞ of
total aprepitant decreased by 42% and Cmax decreased by 32%. Due to modest decreases in protein binding of aprepitant
in patients with renal disease, the AUC of pharmacologically active unbound drug was not significantly affected in
PRIMARY ENDPOINT
patients with renal insufficiency compared with healthy subjects. Hemodialysis conducted 4 or 48 hours after dosinghad no significant effect on the pharmacokinetics of aprepitant; less than 0.2% of the dose was recovered in the dialysate. Complete Response
No dosage adjustment for EMEND is necessary in patients with severe renal insufficiency or in patients with ESRD
OTHER PRESPECIFIED (SECONDARY AND EXPLORATORY) ENDPOINTS Complete Response
Pre-clinical data reveal no special hazard for humans based on conventional studies of single and repeated dose toxicity,genotoxicity, carcinogenic potential, and toxicity to reproduction. However, it should be noted systemic exposure in
rodents was similar or even lower than therapeutic exposure in humans. In particular, although no adverse effects were
noted in reproduction studies at human exposure levels, the animal exposures are not sufficient to make an adequate
Complete Protection III. INDICATIONS
EMEND, in combination with other antiemetic agents, is indicated for the prevention of acute and delayed nausea and
vomiting associated with initial and repeat courses of highly emetogenic cancer chemotherapy, including high-dosecisplatin. No Emesis IV. DOSAGE AND ADMINISTRATION
EMEND is given for 3 days as part of a regimen that includes a corticosteroid and a 5-HT
dose of EMEND is 125 mg orally 1 hour prior to chemotherapy treatment (Day 1) and 80 mg once daily in the morning on
No Nausea
In clinical studies, the following regimen was used:
No Significant Nausea
* EMEND was administered orally 1 hour prior to chemotherapy treatment on Day 1 and in the morning on Days 2 and 3.
N: Number of patients (older than 18 years of age) who received cisplatin, study drug, and had at least one post
**Dexamethasone was administered 30 minutes prior to chemotherapy treatment on Day 1 and in the morning
on Day 2 through 4. The dose of dexamethasone was chosen to account for drug interactions.
Overall: 0 to 120 hours post-cisplatin treatment.
† Ondansetron was administered 30 minutes prior to chemotherapy treatment on Day 1.
Acute phase: 0 to 24 hours post-cisplatin treatment.
Delayed phase: 25 to 120 hours post-cisplatin treatment.
See DRUG INTERACTIONS for additional information on the administration of EMEND with corticosteroids.
Visual analogue scale (VAS) score range: 0 mm = no nausea; 100 mm = nausea as bad as it could be.
Refer to the full prescribing information for coadministered antiemetic agents.
Table 2 includes nominal p-values not adjusted for multiplicity.
EMEND may be taken with or without food.
In both studies, a statistically significantly higher proportion of patients receiving the aprepitant regimen in Cycle 1 had
No dosage adjustment is necessary for the elderly.
a complete response (primary endpoint), compared with patients receiving standard therapy. A statistically significant
No dosage adjustment is necessary based on gender or race.
difference in complete response in favour of the aprepitant regimen was observed when the acute phase and thedelayed phase were analyzed separately.
No dosage adjustment is necessary for patients with severe renal insufficiency (creatinine clearance <30 mL/min) or forpatients with end stage renal disease undergoing hemodialysis.
In both studies, the estimated time to first emesis after initiation of cisplatin treatment was longer with the aprepitantregimen, and the incidence of first emesis was reduced in the aprepitant regimen group compared with standard therapy
No dosage adjustment is necessary for patients with mild to moderate hepatic insufficiency (Child-Pugh score 5 to 9).
group as depicted in the Kapaln-Meier curves in Figure 1.
® REGISTERED TRADEMARK of MERCK & CO., INC., Whitehouse Station, N.J., 08889 U.S.A. Copyright MERCK & CO., INC. 2002
Figure 1: Percent of Patients Who Remain Emesis Free Over Time — Cycle 1 Midazolam: EMEND increased the AUC of midazolam, a sensitive CYP3A4 substrate, by 2.3-fold on Day 1 and 3.3- fold on Day 5, when a single oral dose of midazolam 2 mg was coadministered on Day 1 and Day 5 of a regimen of
EMEND 125 mg on Day 1 and 80 mg/day on Days 2 through 5. The potential effects of increased plasma concentrations
of midazolam or other benzodiazepines metabolized via CYP3A4 (alprazolam, triazolam) should be considered when
coadministering these agents with EMEND.
In another study with intravenous administration of midazolam, EMEND was given as 125 mg on Day 1 and 80 mg/day
on Days 2 and 3, and midazolam 2 mg IV was given prior to the administration of the 3-day regimen of EMEND and on
Days 4, 8, and 15. EMEND increased the AUC of midazolam by 25% on Day 4 and decreased the AUC of midazolam by
19% on Day 8 relative to the dosing of EMEND on Days 1 through 3. These effects were not considered clinically
p-Value <0.001 based on a log rank test for Study 1 and Study 2; nominal p-values not adjusted for multiplicity.
important. The AUC of midazolam on Day 15 was similar to that observed at baseline.
Patient-Reported Outcomes: The impact of nausea and vomiting on patients’ daily lives was assessed in Cycle-1 of
Effect of other agents on the pharmacokinetics of aprepitant
both Phase III studies using the Functional Living Index-Emesis (FLIE), a validated nausea- and vomiting-specific
Aprepitant is a substrate for CYP3A4; therefore, coadministration of EMEND with drugs that inhibit CYP3A4 activity may
patient-reported outcome measure. Minimal or no impact of nausea and vomiting on patient’s Cycle 1 reported no
result in increased plasma concentrations of aprepitant. Consequently, concomitant administration of EMEND with
impact of nausea and vomiting on patients’ daily lives is defined as a FLIE total score >108. In each of the 2 studies, a
strong CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, nefazodone, troleandomycin, clarithromycin, ritonavir, nelfinavir)
higher proportion of patients receiving the aprepitant regimen reported minimal or no impact of nausea and vomiting on
should be approached cautiously; but concomitant administration of EMEND with moderate CYP3A4 inhibitors (e.g.,
daily life (Study 1: 74% versus 64%; Study 2: 75% versus 64%).
diltiazem) does not result in clinically meaningful changes in plasma concentrations of aprepitant.
Multiple-Cycle Extension: In the same 2 clinical studies, patients continued into the Multiple-Cycle extension for up to 5
Aprepitant is a substrate for CYP3A4; therefore, coadministration of EMEND with drugs that strongly induce CYP3A4
additional 6 cycles of chemotherapy. The proportion of patients with no emesis and no significant nausea by treatment
activity (e.g., rifampin, carbamazepine, phenytoin) may result in reduced plasma concentrations of aprepitant that may
group at each cycle is depicted in Figure 2. Antiemetic effectiveness for the patients receiving the aprepitant regimen is
result in decreased efficacy of EMEND. Concomitant administration of EMEND with St. John’s wort is not recommended.
maintained throughout repeat cycles for those patients continuing in each of the multiple cycles. Ketoconazole: When a single 125-mg dose of EMEND was administered on Day 5 of a 10-day regimen of 400 mg/day Figure 2: Percent of Patients With No Emesis and No Significant Nausea by Treatment Group and Cycle
of ketoconazole, a strong CYP3A4 inhibitor, the AUC of aprepitant increased approximately 5-fold and the mean terminalhalf-life of aprepitant increased approximately 3-fold. Concomitant administration of EMEND with strong CYP3A4
inhibitors should be approached cautiously. Rifampin: When a single 375-mg dose of EMEND was administered on Day 9 of a 14-day regimen of 600 mg/day of
rifampin, a strong CYP3A4 inducer, the AUC of aprepitant decreased approximately 11-fold and the mean terminal half-
life decreased approximately 3-fold. Coadministration of EMEND with drugs that induce CYP3A4 activity may result in
reduced plasma concentrations and decreased efficacy of EMEND. Additional interactions Diltiazem: In patients with mild to moderate hypertension, administration of aprepitant once daily, as a tablet formulation
comparable to 230 mg of the capsule formulation, with diltiazem 120 mg 3 times daily for 5 days, resulted in a 2-fold increase
of aprepitant AUC and a simultaneous 1.7-fold increase of diltiazem AUC. These pharmacokinetic effects did not result in
VI. CONTRAINDICATIONS
clinically meaningful changes in ECG, heart rate, or blood pressure beyond those changes induced by diltiazem alone.
EMEND is contraindicated in patients who are hypersensitive to any component of the product. Paroxetine: Coadministration of once daily doses of aprepitant, as a tablet formulation comparable to 85 mg or 170 mg
EMEND should not be used concurrently with pimozide, terfenadine, astemizole, or cisapride. Inhibition of cytochrome
of the capsule formulation, with paroxetine 20 mg once daily, resulted in a decrease in AUC by approximately 25% and
P450 isoenzyme 3A4 (CYP3A4) by aprepitant could result in elevated plasma concentrations of these drugs, potentially
Cmax by approximately 20% of both aprepitant and paroxetine.
causing serious or life-threatening reactions (see DRUG INTERACTIONS). XIII. SIDE EFFECTS VII. PRECAUTIONS
The overall safety of aprepitant was evaluated in approximately 3300 individuals.
EMEND should be used with caution in patients receiving concomitant medicinal products that are primarily metabolized
In 2 well-controlled clinical trials in patients receiving highly emetogenic cancer chemotherapy, 544 patients were treated
through CYP3A4; some chemotherapy agents are metabolized by CYP3A4 (see DRUG INTERACTIONS). Caution is
with aprepitant during Cycle 1 of chemotherapy and 413 of these patients continued into the Multiple-Cycle extension
advised both during and up to 2 weeks after the end of treatment with EMEND due to the inhibitory and inductive effects
for up to 6 cycles of chemotherapy. EMEND was given in combination with ondansetron and dexamethasone (aprepitant
of aprepitant on CYP3A4 substrates. Inhibition of CYP3A4 by aprepitant could result in elevated plasma concentrations
regimen) and was generally well tolerated. Most adverse experiences reported in these clinical studies were described
of these concomitant medicinal products (see DRUG INTERACTIONS).
Coadministration of EMEND with ergot alkaloid derivatives, which are CYP3A4 substrates, may result in elevated
In Cycle 1, drug-related clinical adverse experiences were reported in approximately 17% of patients treated with the
plasma concentrations of these medicinal products. Therefore, caution is advised due to potential risk of ergot-related
aprepitant regimen compared with approximately 13% of patients treated with standard therapy. Aprepitant was
discontinued due to drug-related clinical adverse experiences in 0.6% of patients treated with the aprepitant regimen
Chronic continuous use of EMEND for prevention of nausea and vomiting is not recommended because it has not been
compared with 0.4% of patients treated with standard therapy.
studied and because the drug interaction profile may change during chronic continuous use.
The most common drug-related adverse experiences reported in patients treated with the aprepitant regimen were: hiccups
Coadministration of EMEND with warfarin results in decreased prothrombin time, reported as International Normalized
(4.6%), asthenia/fatigue (2.9%), ALT increased (2.8%), constipation (2.2%), headache (2.2%), and anorexia (2.0%).
Ratio (INR). In patients on chronic warfarin therapy, the prothrombin time (INR) should be closely monitored to establish
The following drug-related adverse experiences were observed in patients treated with the aprepitant regimen and at a
and maintain the required dose of warfarin, in the 2 weeks period, particularly at 7-10 days, following initiation of the 3-
day regimen of EMEND with each chemotherapy cycle (see DRUG INTERACTIONS).
[Common (>1/100, <1/10) Uncommon (>1/1000, <1/100)]
The efficacy of oral contraceptives during chronic administration of EMEND may be reduced. Although a 3-day regimen
Blood and the lymphatic system disorders:
of EMEND given concomitantly with oral contraceptives has not been studied, alternative or back-up methods of
contraception should be used during treatment with EMEND and for 2 months following the last dose of EMEND. (see
Metabolism and nutrition disorders:
Patients with rare hereditary problems of fructose intolerance, glucose-galactose malabsorption or sucrase-isomaltase
insufficiency should not take this medicine. Psychiatric disorders: VIII. PREGNANCY
There are no adequate and well-controlled studies in pregnant women. EMEND should be used during pregnancy only,
Nervous system disorders:
if the potential benefit justifies the potential risk to the mother and the fetus. IX. NURSING MOTHERS Eye disorders:
Aprepitant is excreted in the milk of lactating rats. It is not known whether this drug is excreted in human milk. Because
many drugs are excreted in human milk and because of the possible adverse effects of EMEND on nursing infants, a
Ear and labyrinth disorders:
decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance
Cardiac disorders: X. PEDIATRIC USE
Safety and effectiveness of EMEND in pediatric patients have not been established. Use in patients under 18 years of
Respiratory, thoracic and mediastinal disorders: XI. USE IN THE ELDERLY
In clinical studies, the efficacy and safety of EMEND in the elderly (≥65 years) were comparable to those seen in
Gastrointestinal disorders:
younger patients (<65 years). No dosage adjustment is necessary in elderly patients.
Common: constipation, diarrhea, dyspepsia
XII. DRUG INTERACTIONS
Uncommon: nausea, acid reflux, dysgeusia, epigastric discomfort, obstipation, gastroesophageal reflux disease, perforating
Aprepitant is a substrate, a moderate inhibitor, and an inducer of CYP3A4. Aprepitant is also an inducer of CYP2C9.
duodenal ulcer, vomiting. Skin and subcutaneous tissue disorders: Effect of aprepitant on the pharmacokinetics of other agents
Uncommon: rash, acne, photosensitivity.
As a moderate inhibitor of CYP3A4, aprepitant can increase plasma concentrations of coadministered medicinal products
Renal and urinary disorders:
that are metabolized through CYP3A4.
EMEND should not be used concurrently with pimozide, terfenadine, astemizole, or cisapride. Inhibition of CYP3A4 by
General disorders and administration site conditions:
aprepitant could result in elevated plasma concentrations of these drugs, potentially causing serious or life-threatening
Uncommon: abdominal pain, edema, flushing.
Aprepitant has been shown to induce the metabolism of S(-) warfarin and tolbutamide, which are metabolized through
Investigations:
CYP2C9. Coadministration of EMEND with these drugs or other drugs that are known to be metabolized by CYP2C9,
such as phenytoin, may result in lower plasma concentrations of these drugs.
Uncommon: alkaline phosphatase increased, hyperglycemia, microscopic hematuria, hyponatremia.
EMEND is unlikely to interact with drugs that are substrates for the P-glycoprotein transporter, as demonstrated by the
The adverse experience profile in the Multiple-Cycle extension for up to 6 cycles of chemotherapy was generally similar
lack of interaction of EMEND with digoxin in a clinical drug interaction study.
In other clinical studies, isolated cases of serious adverse experiences were reported. Stevens-Johnson syndrome was
3 antagonists: In clinical drug interaction studies, aprepitant did not have clinically important effects on the
pharmacokinetics of ondansetron or granisetron. No clinical or drug interaction study was conducted with dolasetron.
reported in a patient receiving aprepitant with cancer chemotherapy in another chemotherapy-induced nausea andvomiting (CINV) study. Angioedema and urticaria were reported in a patient receiving aprepitant in a non-CINV study. Corticosteroids: Dexamethasone: EMEND, when given as a regimen of 125 mg with dexamethasone coadministered orally as 20 mg on XIV. OVERDOSAGE
Day 1, and EMEND when given as 80 mg/day with dexamethasone coadministered orally as 8 mg on Days 2 through 5,
No specific information is available on the treatment of overdosage with EMEND. Single doses up to 600 mg of aprepitant
increased the AUC of dexamethasone, a CYP3A4 substrate by 2.2-fold, on Days 1 and 5. The usual oral dexamethasone
were generally well tolerated in healthy subjects. Aprepitant was generally well tolerated when administered as 375 mg
doses should be reduced by approximately 50% when coadministered with EMEND, to achieve exposures of
once daily for up to 42 days to patients in non-CINV studies. In 33 cancer patients, administration of a single 375-mg
dexamethasone similar to those obtained when it is given without EMEND. The daily dose of dexamethasone administered
dose of aprepitant on Day 1 and 250 mg once daily on Days 2 to 5 was generally well tolerated.
in clinical studies with EMEND reflects an approximate 50% reduction of the dose of dexamethasone (see DOSAGE
Drowsiness and headache were reported in one patient who ingested 1440 mg of aprepitant.
In the event of overdose, EMEND should be discontinued and general supportive treatment and monitoring should be
Methylprednisolone: EMEND, when given as a regimen of 125 mg on Day 1 and 80 mg/day on Days 2 and 3, increased
provided. Because of the antiemetic activity of aprepitant, drug-induced emesis may not be effective.
the AUC of methylprednisolone, a CYP3A4 substrate, by 1.3-fold on Day 1 and by 2.5-fold on Day 3, when
Aprepitant cannot be removed by hemodialysis.
methylprednisolone was coadministered intravenously as 125 mg on Day 1 and orally as 40 mg on Days 2 and 3. Theusual IV methylprednisolone dose should be reduced by approximately 25%, and the usual oral methylprednisolone
XV. STORAGE
dose should be reduced by approximately 50% when coadministered with EMEND, to achieve exposures of
STORAGE CONDITION: Store at or below 30°C (88°F)
methylprednisolone similar to those obtained when it is given without EMEND. XVI. SHELF LIFE Chemotherapeutic agents: In clinical studies, EMEND was administered with the following chemotherapeutic agents
Please refer to the expiry date on the carton.
metabolized primarily or in part by CYP3A4: etoposide, vinorelbine, docetaxel, paclitaxel, irinotecan, ifosfamide, imatinib,
XVII. AVAILABILITY
vinblastin and vincristine. The doses of these agents were not adjusted to account for potential drug interactions. Packaging:
However, caution is advised and additional monitoring may be appropriate in patients receiving such agents (see
Treatment (or Multiple)-pack:
EMEND is packaged in a tri-fold pack containing 1 capsule of EMEND 125mg & 2 capsules of EMEND 80mg. Warfarin: A single 125-mg dose of EMEND was administered on Day 1 and 80 mg/day on Days 2 and 3 to healthy
subjects who were stabilized on chronic warfarin therapy. Although there was no effect of EMEND on the plasma AUC
EMEND 80mg Capsule: White, opaque hard gelatin capsule with “461” and “80mg” printed radially in black ink.
of R(+) or S(-) warfarin determined on Day 3, there was a 34% decrease in S(-) warfarin (a CYP2C9 substrate) trough
EMEND 125mg Capsule: Opaque hard gelatin capsule with white body and pink cap, with “462” and “125mg” printed
concentration accompanied by a 14% decrease in the prothrombin time (reported as International Normalized Ratio or
INR) 5 days after completion of dosing with EMEND. In patients on chronic warfarin therapy, the prothrombin time (INR)
MANUFACTURER
should be closely monitored in the 2-week period, particularly at 7 to 10 days following initiation of the 3-day regimen of
Sumneytown Pike, West Point, 19486 PA, USA. Tolbutamide: EMEND, when given as 125 mg on Day 1 and 80 mg/day on Days 2 and 3, decreased the AUC of
tolbutamide (a CYP2C9 substrate) by 23% on Day 4, 28% on Day 8, and 15% on Day 15, when a single dose of tolbutamide
Merck Sharp & Dohme (Aus) Pty. Ltd.
500 mg was administered orally prior to the administration of the 3-day regimen of EMEND and on Days 4, 8, and 15.
54-68 Ferndell Street, South Granville, NSW 2142, AUSTRALIA
Oral contraceptives: Aprepitant, when given once daily for 14 days as a 100-mg capsule with an oral contraceptive IMPORTER
containing 35 mcg of ethinyl estradiol and 1 mg of norethindrone, decreased the AUC of ethinyl estradiol by 43%, and
Merck Sharp & Dohme (I.A.) Corp., Malaysia Branch
decreased the AUC of norethindrone by 8%; therefore the efficacy of oral contraceptives during administration of EMEND
Letter Box 1502, 15th Floor, Menara Merais, No. 1, Jalan 19/3, 46300 Petaling Jaya, Selangor, MALAYSIA
may be reduced. Although a 3-day regimen of EMEND given concomitantly with oral contraceptives has not beenstudied, alternative or back-up methods of contraception should be used.
When will an IP valuation be helpful in inform-Tim Heberden BRAND FINANCE AUSTRALIA Tax planning Intellectual property valuations can inform a range of legalMany multinationals are structuring their IP in spe-issues, including commercialisation, licensing, litigation,cialist IP-holding companies (IPCos) for commercialtransfer pricing, IP audits and mergers and acquisitionsand tax re
Julia Hughes HNC/D Animal Studies Module: Microbiology Microbiology: Practical Competence Introduction Infectious diseases in animals are caused by the invasion of tissues by bacteria, especially the epithelium, by microorganisms. This invasion have many effects which can be detrimental to the animals health, let alone be passed on to other animals through physical contact,
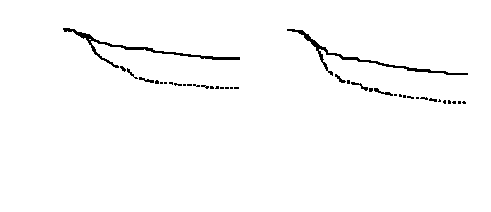 Figure 1: Percent of Patients Who Remain Emesis Free Over Time — Cycle 1
Figure 1: Percent of Patients Who Remain Emesis Free Over Time — Cycle 1