Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Microsoft word - initialintakeform
Welcome to our clinic. Please help up provide you with the best care by taking time to complete this evaluation questionnaire. All answers will be held absolutely CONFIDENTIAL. If you have any questions please feel free to ask. If there is anything you wish to bring to our attention which is not asked in this form please use the ‘Comments’ section. Thank you.
Personal Information
Name______________________________________________________ Date___________________________ Home Address _______________________________________________________________________________ City______________________________________________ State__________________ Zip______________ Home Phone_________________________________ Work Phone____________________________________ Cell Phone ___________________________ E-mail _______________________________________________ Occupation______________________ Family Physician ____________________________________________ In Emergency Notify_________________________ Phone___________________ Relationship ______________ Who should we thank for referring you to this office? ________________________________________________ Sex: □ Male □ Female
Height_______ Weight_______ Birth date__________ Age____
Marital Status: Married___ Single___ Divorced___ Widowed___ Number of children____ Have you received acupuncture therapy before? □ Yes □ No When?______With whom?_______ Past Medical history/Family History
Illness
Cancer ____ ____ ________ Diabetes ____ ____ ________ Hepatitis ____ ____ ________ Heart Disease ____ ____ ________ High blood pressure ____ ____ ________ Seizures ____ ____ ________ Rheumatic Fever ____ ____ ________ Emotional Disorders ____ ____ ________ Infectious Disease ____ ____ ________ Tuberculosis ____ ____ ________ Sexually Transmitted Diseases: □ Gonorrhea □ Syphilis □ AIDS □ HPV □ Chlamydia □ Herpes Date _______________ Other relevant medical history (please include dates) _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ List any medications and/or supplements you are currently taking (continue on the back if necessary) Medicine and Dosage Check the appropriate box if any of the following statements are true:
□ I am taking lithium (Eskalith, Lithobid, Lithonate, Lithotabs)
Please indicate the use and frequency of the following:
What is/are the main health problem(s) for which you are seeking treatment? ________________________________________________________________________________________ __________________________________________________________________________________ To what extend does this problem affect your daily activities (work, sleep, eating, etc.)?_______________ _____________________________________________________________________________________ How long has it been since you first noticed any symptoms? ____________________________________ Have you been given a diagnosis for this problem by a family physician? __________________________
If so, what is it?__________________________________________________________________
What other forms of treatment have you sought? ________________________________________________________________________________________ __________________________________________________________________________________ List any allergies, food sensitivities or food cravings that you have. ________________________________________________________________________________________ __________________________________________________________________________________ List any accidents, surgeries, or hospitalizations (include date). ________________________________________________________________________________________ ________________________________________________________________________________________ Occupational stressfactors (physical, psychological, chemical): ___________________________________ Lab Results (please include copies) _____________________________________________________________________________________ How do you feel about the following areas of your life? (please check the appropriate spaces and indicate any problems you may be experiencing) Great Significant Exercise Spirituality
Your Comments (use back if necessary): ___________________________________________________________ _____________________________________________________________________________________________ For Women Age of first period (menarche)________ Are you pregnant? □ Yes □ No # of pregnancies _____ # of live births____ Age of last period (menopause)_______
# of abortions _____ # of miscarriages ____
Number of days between periods______ Date of last: Gynecologic exam _____________ Pap smear ____________ Number of days of flow_____________
Mammogram________________ Bone Density scan ____________________
Results _________________________________________________________
Color of flow: _______ Spotting? □ Yes □ No Average number of pads you use per day: 1st day____ 2nd day____ 3rd day____ 4th day_____ + days_____ Have you been diagnosed with: □ Fibroids □ Fibrocystic Breasts □ Endometriosis □ Ovarian cysts PID____
Location of pain: Lower abdomen___ Lower back___ Thighs___ Other__________ Nature of pain (please indicate before, during or after menses): Other symptoms related to menses:
□ Swollen Breasts □ Mood swings □ Ravenous appetite
Bloating □yes □no □ Poor appetite □ Hot flashes □ Night sweats
Bearing down sensation __________________________
□ Increased libido □ Decreased libido □ Insomnia
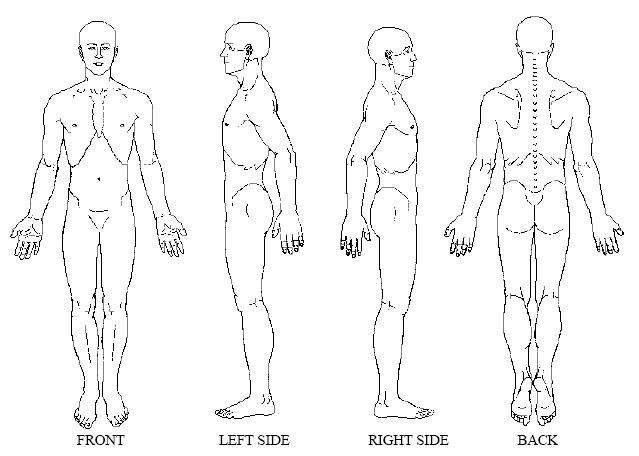
For Men Date of last prostate check up __________ PSA results___________ Manual prostate exam results_______________________ Lab Results: _____________________________________________________________________________________________ Frequency of Urination: daytime _____ Nighttime______ Color of urine: □ clear □ murky Odor: ________________________ Symptoms related to prostate: □ Erectile Dysfunction □ Increased Libido Pain chart
please mark painful or areas of distress on the chart below (use words if necessary)
. Symptom Survey
The following is a list of symptoms that you have experienced within the last three months. Indicate the length of time you have had this condition. Please indicate as follows: blank = never experience check mark (√) = sometimes experience plus sign (+) = frequently experience □ Insomnia: __ Difficulty going to sleep __ Difficulty waking up __ Difficulty staying asleep □ Emotional state: __ Happy __ Sad __Angry __Depressed __Over thinker __Lethargic □ Circulatory Problems: __Cold Hands __Cold Feet __Both __Other: Describe_________________________________________ □ Palpitations: How often _____________ Under what conditions ___________________________________________________ □ Appetite: __Increased __Decreased __Easily Hungered __No Appetite □ Bloating □ Gas □ Acid Reflux □ Indigestion □ Diarrhea □ Constipation □ Abdominal aches/pains □ Respiratory problems □ Cough: __Dry __Wet __Cough up Phlegm □ Shortness of Breath: __Slight Exertion __All the time □ Asthma: __Mild __Intermittent __Chronic When were you diagnosed______________________________________________ □ Stifling sensation in chest □ Allergies □ Sinus Problems □ Easily catch cold □ Urination problem Describe__________________________________________________________________________________ □ Painful Urination □ Night urination □ Easily Agitated □ Difficulty Making Decisions □ Headaches: How often _______________ Location______________________________________________________________ □ Bitter Taste in mouth □ Dry Eyes □ Brittle Nails □ Stiff Joints In general, do you feel more ____Hot or more ____Cold Are you thirsty ____No ____Yes How many hours do you sleep per night _____________________ How is your overall energy level______________________________________________________________________________ Any recent changes in vision ___No ____Yes Do you see floaters in your vision ___No ___Yes Any recent changes in your hearing ___No ____Yes Please Describe
_______________________________________________________
Any other abnormal conditions that you have noticed in your general sense of health _____________________________________
CONDI| II COMERCIALE GENERALE PENTRU LEASING FINANCIAR DOBÂND{ FIX{ - PERSOANE FIZICE Articolul 2. Dreptul de proprietate. Paza juridic[ Articolul 3. Livrare. Înmatriculare. Perioada de leasing. Durata contractului Articolul 4. Avansul. Diferen\e de curs valutar privind Volumul Finan\at Articolul 5. Dobânda de leasing. Dobânda anual[ efectiv[. Costuri majorate Articolul 6. Rate de

 For Women
For Women