Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Sonometrics.net
Ventricular interaction and external constraint accountfor decreased stroke work during volume loading in CHF
THOMAS D. MOORE,1 MICHAEL P. FRENNEAUX,1 ROZSA SAS,2J. J. ATHERTON,3 JAYNE A. MORRIS-THURGOOD,1 ELDON R. SMITH,2JOHN V. TYBERG,2 AND ISRAEL BELENKIE22Departments of Medicine and Physiology and Biophysics, University of Calgary,Calgary, Alberta T2N 4N1, Canada; 3University of Queensland, Brisbane Q4029, Australia;and 1Department of Cardiology, Wales Heart Research Institute,University of Wales College of Medicine, Cardiff CF14 4XN, United Kingdom
Received 26 April 2001; accepted in final form 13 August 2001
Moore, Thomas D., Michael P. Frenneaux, Rozsa Sas,
capillary wedge pressure (PCWP) is reduced (4, 28) at
J. J. Atherton, Jayne A. Morris-Thurgood, Eldon R.
first sight seem to suggest that volume manipulation
Smith, John V. Tyberg, and Israel Belenkie. Ventricular
may alter contractility and that there is a descending
interaction and external constraint account for decreased
limb of the SW-LVEDV (Starling) relation.
stroke work during volume loading in CHF. Am J Physiol
The effective LV distending pressure is transmural LV
Heart Circ Physiol 281: H2385–H2391, 2001.—The slope of
end-diastolic pressure (LVEDP), which is LVEDP minus
the stroke work (SW)-pulmonary capillary wedge pressure
the surrounding [pericardial and right ventricular (RV)]
(PCWP) relation may be negative in congestive heart failure
pressure. Normally, pericardial pressure and RV end-
(CHF), implying decreased contractility based on the premisethat PCWP is simply related to left ventricular (LV) end-
diastolic pressure (EDP) are low, but in some conditions,
diastolic volume. We hypothesized that the negative slope is
may be markedly elevated. In these situations, the pres-
explained by decreased transmural LV end-diastolic pressure
sure surrounding the LV may contribute substantially to
(LVEDP), despite the increased LVEDP, and that contractil-
measured LVEDP (7), and the effective distending pres-
ity remains unchanged. Rapid pacing produced CHF in six
sure may be considerably lower than the measured
dogs. Hemodynamic and dimension changes were then mea-
LVEDP. It is now also clear that in these situations,
sured under anesthesia during volume manipulation. Vol-
changes in LVEDP may not accurately reflect changes in
ume loading increased pericardial pressure and LVEDP but
the effective distending pressure (transmural LVEDP).
decreased transmural LVEDP and SW. Right ventricular
In a model of acute pulmonary embolism (4, 5), volume
diameter increased and septum-to-LV free wall diameter
loading decreased SW despite the increased LVEDP; the
decreased. Although the slopes of the SW-LVEDP relations
opposite occurred during volume removal. This apparent
were negative, the SW-transmural LVEDP relations re-
paradox of decreased cardiac function when filling pres-
mained positive, indicating unchanged contractility. Simi-
sure is increased did not represent decreased contractil-
larly, the SW-segment length relations suggested unchanged
ity; rather, it was explained by a greater increase in
contractility. Pressure surrounding the LV must be sub-
pericardial pressure and RVEDP than the increase in
tracted from LVEDP to calculate transmural LVEDP accu-rately. When this was done in this model, the apparent
LVEDP. This resulted in a reduction in transmural
decrease in contractility was no longer evident. Despite the
LVEDP and thus decreased LVEDV; the decreased
increased LVEDP during volume loading, transmural
LVEDV was responsible for the reduced SW in keeping
LVEDP and therefore SW decreased and contractility re-
with Starling’s Law despite the increased intracavitary
LVEDP. The reverse was true during volume removal. Similar observations were made in patients with chronic
congestive heart failure; hemodynamics; pericardium
obstructive pulmonary disease in whom volume loadingdecreased LVEDV despite increased PCWP (17).
Data from two studies suggest that a similar phe-
IT IS IMPORTANT TO ASSESS the hemodynamic status accu-
nomenon may also occur in congestive heart failure. In
rately in congestive heart failure and to understand
some patients, LVEDV increased during nitroglycerin
how treatment affects left ventricular (LV) end-dia-
administration or when central blood volume was re-
stolic volume (LVEDV) because cardiac function is in
duced with lower body negative pressure, despite the
part dependent on preload. The old observation that
fact that both interventions decrease LVEDP (3, 9). We
phlebotomy increased cardiac output as central venous
suggested previously (2) that these findings can be
pressure fell (16) and the more recent observations
explained by decreased constraint to LV filling and
that stroke work (SW) may increase as pulmonary
The costs of publication of this article were defrayed in part by the
Address for reprint requests and other correspondence: I. Belen-
payment of page charges. The article must therefore be hereby
kie, Health Sciences Center, 3330 Hospital Dr. NW, Calgary, Al-
marked ‘‘advertisement’’ in accordance with 18 U.S.C. Section 1734
berta, Canada T2N4N1 (E-mail: [email protected]).
0363-6135/01 $5.00 Copyright 2001 the American Physiological Society
direct ventricular interaction. However, there are no
five animals, four from over the LV; pressure from over the RV
published studies in which simultaneous cardiac func-
was used in one animal because of unsuitable tracings over the
tion, pressures, and dimensions were measured to ver-
LV. In dog 6, pericardial pressures were technically unaccept-
ify that constraint to filling and ventricular interaction
able, and right atrial pressure was used as an approximation tocalculate transmural LVEDP. In dog 1, catheter whip from the
are responsible for the apparent paradoxical response
pericardial transducer sometimes caused too much artifact so
to volume loading in congestive heart failure.
that only the cardiac cycles just before, at, and just after end
Using the canine rapid-pacing congestive heart fail-
expiration were used to calculate transmural LVEDP. Data
ure model, we tested the hypothesis that volume load-
collected during volume removal in three dogs were excluded
ing may decrease and volume removal may increase
because of severe hemodynamic deterioration (systolic aortic
transmural LVEDP, despite opposite changes in intra-
pressure decreased rapidly to Ͻ70 mmHg and SV decreased to
cavitary LVEDP, and that changes in SW would par-
Ͻ50%). Transmural LVEDP was calculated as LVEDP Ϫ peri-
allel changes in transmural LVEDP. We also hypoth-
cardial pressure. The transseptal pressure gradient was calcu-
esized that, as in pulmonary embolism and chronic
lated as LVEDP Ϫ RVEDP. SW was calculated as SV ϫ (LV
pulmonary disease, ventricular interaction would ac-
end-systolic pressure Ϫ LVEDP) (expressed in mmHg⅐ml). End-diastolic dimensions were measured at the peak of the R wave
count for the associated changes in ventricular dimen-
sions. Our results confirm that changes in intracavitary
Statistical analysis. Hemodynamic and dimension changes
LVEDP may not reliably predict changes in transmural
during volume loading were compared with the Student’s
LVEDP in severe congestive heart failure; our results
paired t-test. A probability Ͻ0.05 was considered to be sta-
also clarify the mechanism by which this occurs.
In the four awake dogs in which PCWP was mea-
Experimental model. Rapid ventricular pacing (220–250
beats/min for 4–6 wk) produced severe congestive heart failure
sured, mean PCWP fell from a mean of 25 (range
(severe LV dysfunction observed echocardiographically, associ-
16–37) mmHg before anesthesia to 16 (range 5–34)
ated with lassitude, dyspnea, and ascites) in six dogs (both
mmHg when first measured under anesthesia with the
sexes, 20–25 kg) as previously described (2, 11, 14, 15, 29, 32).
chest open and the pericardium closed. After instru-
The pacemakers were then turned off, and the dogs were stud-
mentation and stabilization with variable amounts of
ied acutely. (Four were first placed in a supporting sling and,
fluid in all six anesthetized animals, LVEDP was
with the use of local anesthesia, a catheter was advanced to the
pulmonary artery to measure PCWP.) Anesthesia was then
Volume loading. Table 1 lists the hemodynamic and
induced with intravenous fentanyl citrate (0.1 mg/ml) followed
dimension data at baseline and during volume manip-
by ϳ2 mg/kg Pentothal Sodium. The animals were then venti-lated with a 70% nitrous oxide-30% oxygen mixture with aconstant-volume respirator. Anesthesia was maintained with
Table 1. Hemodynamic and dimension changes
fentanyl at a rate of ϳ4 mg/h. A midline sternotomy was
during volume manipulation in heart failure
performed, the pericardium was incised along the base of theventricles, and the heart was removed from the sac for instru-
mentation (4). LV, aortic, and RV pressures were measured
with 8-Fr catheter-tipped transducers (model SPC-485A, MillarInstruments; Houston, TX) inserted through a carotid artery
and a femoral artery and vein, respectively. Right atrial pres-
sure was measured with a fluid-filled catheter inserted through
a jugular vein. Pericardial pressure was measured over the
lateral surface of both ventricles with flat, fluid-filled balloon
transducers (13). Septum-to-LV free wall, LV anteroposterior,
and septum-to-RV free wall diameters, as well as LV free wall
segment length were measured by sonomicrometry (Sonomet-
rics, London, Ontario, Canada). An ultrasonic flow probe (Tran-
sonic Systems; Ithaca, NY) was implanted on the aorta to
measure stroke volume (SV). A signal from the respirator was
used to identify end-expiratory cardiac cycles, and a single lead
electrocardiogram was recorded. The pericardium and chest
were closed, and the animals were stabilized.
Data are means Ϯ SD from all dogs are available during volume
Experimental protocol. While data were continuously col-
loading but in only 3 animals during volume removal because of hemo-
lected, volume loading was performed with 200–750 ml hep-
dynamic instability in the two remaining dogs. HR, heart rate (beats/
arinized saline or a solution of 25 mg/l albumin over 1–4 min
min); LVAP, left ventricular (LV) anteroposterior diameter (mm);
until the LVEDP was at least 35 mmHg or hemodynamic
LVEDP, LV end-diastolic pressure (mmHg); LVSP, peak LV systolic
instability developed. Volume was then removed over a sim-
pressure (mmHg); PerP, pericardial pressure (mmHg); RVEDP, right
ilar period of time to either reduce the LVEDP to 12 mmHg
ventricular (RV) end-diastolic pressure (mmHg); RVSP, peak RV sys-tolic pressure (mmHg); SegL, Segment length (mm); SLVFW, septum-
or the systolic aortic pressure to Ͻ75 mmHg. The blood-
to-LV free wall diameter (mm); SRVFW, septum-to-RV free wall diam-
saline mixture was then reinfused until the LVEDP was the
eter (mm); SV, stroke volume (ml); SW, stroke work (ml⅐mmHg).
same as at the start of the protocol.
TLVEDP, transmural LVEDP (mmHg); TSG, transseptal pressure gra-
Data analysis. Data collected throughout respiration were
dient (mmHg); Data collected during volume removal were not sub-
analyzed. Pericardial pressure measurements were available in
jected to statistical analysis. *P Ͻ 0.01; †P Ͻ 0.05. AJP-Heart Circ Physiol • VOL 281 • DECEMBER 2001 • www.ajpheart.org
ulation. Figure 1 illustrates the changes in pressures,LV performance, and dimensions during volume load-ing and removal in a representative dog (dog 5). Vol-ume loading increased LVEDP (from 20.9 Ϯ 1.8 to26.8 Ϯ 2.9 mmHg) but increased RVEDP more (from15.1 Ϯ 1.6 to 24.3 Ϯ 2.3 mmHg), thus decreasing thetransseptal pressure gradient (from 6.4 Ϯ 1.1 to 3.0 Ϯ1.1 mmHg). As shown in Fig. 2, the increase in peri-cardial pressure during volume loading (from 13.6 Ϯ1.9 to 21.8 Ϯ 3.2 mmHg) was similar to the increase inRVEDP. The decrease in transmural LVEDP (from6.6 Ϯ 0.7 to 4.5 Ϯ 1.1 mmHg) was similar to thedecrease in the transseptal pressure gradient. Thedecreased transseptal pressure gradient and transmu-ral LVEDP were associated with a decreased SV (from11.7 Ϯ 2.8 to 10.1 Ϯ 2.6 ml) and SW (from 418 Ϯ 101 to291 Ϯ 78 ml ⅐ mmHg). All of the above changes werestatistically significant. The changes in peak LV sys-tolic pressure, peak RV systolic pressure, and heartrate were not significant. Volume removal. The data are from the three ani-
mals that remained hemodynamically stable duringvolume removal. As illustrated in Fig. 1 and listed inTable 1, volume removal reversed the changes causedby volume loading. As LVEDP decreased (from 29.3 Ϯ
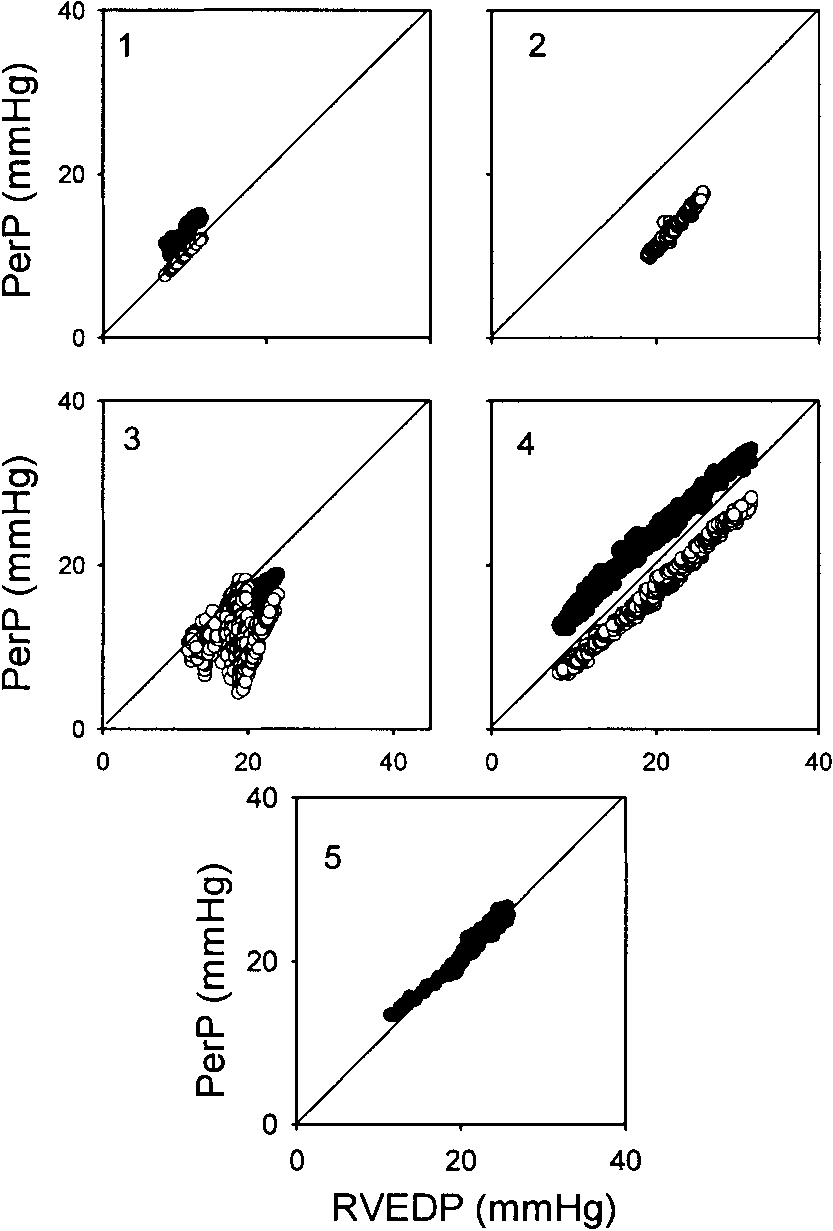
Fig. 2. Plots of PerP versus RVEDP. PerP measurements over bothventricles were available and similar in 3 dogs (dogs 1, 3 and 4) asindicated by open and closed circles. Changes in PerP were closelyrelated to changes in RVEDP. PerP was not available in dog 6. SeeFig. 1 for abbreviations.
2.6 to 23.3 Ϯ 2.6 mmHg), there was also a decrease inRVEDP (from 22.7 Ϯ 1.9 to 14.7 Ϯ 2.7 mmHg), result-ing in an increased transseptal pressure gradient (from6.7 Ϯ 4.3 to 8.7 Ϯ 3.5 mmHg). The decrease in pericar-dial pressure (24.7 Ϯ 0.3 to 16.7 Ϯ 2.4 mmHg) wassimilar to that in RVEDP. Transmural LVEDP in-creased (from 4.7 Ϯ 2.9 to 6.7 Ϯ 2.0 mmHg) and SV andSW increased from 15.3 Ϯ 4.0 to 16.5 Ϯ 5.2 ml and483 Ϯ 143 to 593 Ϯ 167 mmHg ⅐ ml, respectively. PeakLV systolic pressure and heart rate remained un-changed, and peak RV systolic pressure decreasedslightly from 37.3 Ϯ 1.5 to 35.0 Ϯ 1.7 mmHg. Effects of volume manipulation on dimensions. As
illustrated in Fig. 1 and listed in Table 1, changes inthe transseptal pressure gradient caused the septum toshift predictably. During volume loading, the de-creased transseptal pressure gradient caused a left-ward septal shift [the septum-to-LV free wall diameter
Fig. 1. Hemodynamic and dimension changes during volume loading
decreased from 50.5 Ϯ 1.4 to 49.8 Ϯ 1.3 mm (P Ͻ 0.05),
and removal in a representative animal (dog 5). Top: changes in left
and the septum-to-RV free wall diameter increased
ventricular (LV) and right ventricular (RV) end-diastolic pressure
from 42.7 Ϯ 4.8 to 44.4 Ϯ 4.7 mm (P Ͻ 0.01)]. The
(EDP), pericardial pressure (PerP), transseptal pressure gradient
increased transseptal pressure gradient during volume
(TSG), and transmural LVEDP (TLVEDP). Middle: changes instroke volume (SV) and stroke work (SW). Bottom: changes in cham-
removal caused a rightward septal shift in all three
ber dimensions. As LVEDP increased during loading, RVEDP and
animals (septum-to-LV free wall diameter increased
PerP increased more so that the TSG and TLVEDP decreased. These
from 51.0 Ϯ 2.1 to 51.5 Ϯ 1.7 mm and the RV dimen-
changes were associated with a decrease in SV and SW, decreased
sion decreased from 45.5 Ϯ 8.7 to 43.9 Ϯ 8.8 mm).
septum-to-LV free wall diameter (SLVFW), and increased septum-
There was no significant change in segment length
to-RV free wall diameter (SRVFW). Changes were reversed duringvolume removal. AJP-Heart Circ Physiol • VOL 281 • DECEMBER 2001 • www.ajpheart.org
LV segment length. Figure 3 shows the LVEDP- and
transmural LVEDP-segment length relations in eachanimal. As can be seen, transmural LVEDP was con-sistently lower than LVEDP and segment length wasmore closely related to transmural LVEDP thanLVEDP. There was little change in segment length indog 4, and there was little change in pressure in dog 1. In four dogs (dogs 3–6), there was considerably morescatter in the LVEDP-segment length relations. LV function. The SW-LVEDP relations (Fig. 4A) in
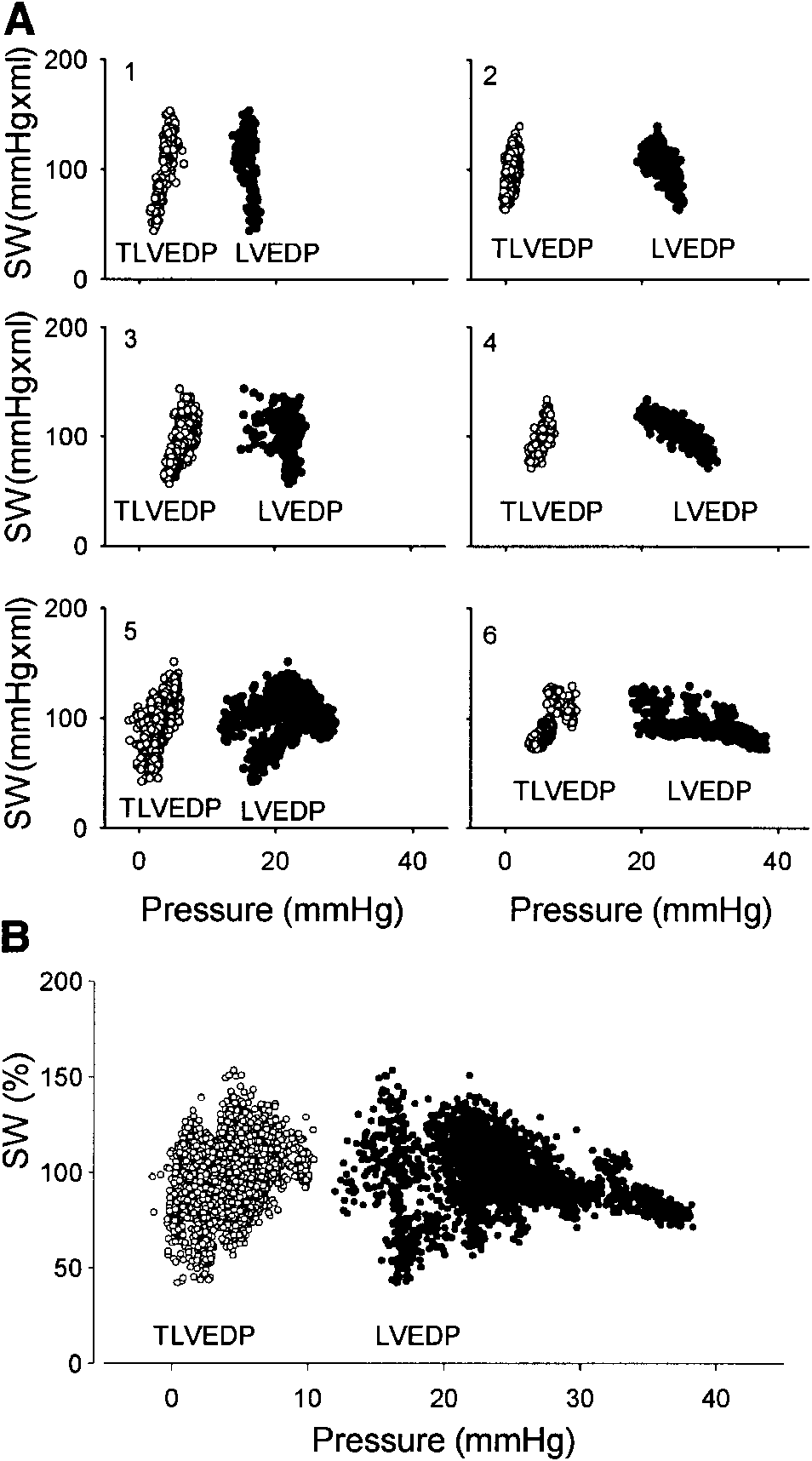
each animal were negative and, if interpreted in theconventional manner, imply that contractility de-creased as LVEDP increased. However, the SW-trans-mural LVEDP relations were positive in all animals,SW consistently increasing as a function of increasingtransmural LVEDP. Figure 4B shows the summarydata from all animals in which SW was normalized(100% equals the average of the highest and lowestvalue for each dog). The SW-LVEDP plots showedconsiderably more scatter than the SW-transmuralLVEDP plots. Figure 5 shows the SW-end-diastolicsegment length relations in each dog. In three dogs, theSW-segment length relations had a positive slope,whereas there was little change in segment length inone dog (dog 4) and in SW in another dog (dog 1). Pericardial constraint. Pericardial pressure varied
considerably between animals and during volume ma-nipulation (Table 1). However, as illustrated in Fig. 2,pericardial pressure was similar to RVEDP, andchanges in pericardial pressure (from 13.6 Ϯ 1.9 to21.8 Ϯ 3.2 mmHg, P Ͻ 0.01) during volume loadingwere similar to those in RVEDP (from 15.1 Ϯ 1.6 to24.3 Ϯ 2.3 mmHg, P Ͻ 0.01) throughout the range offilling pressures in the five animals in which it wasobtained. Transmural RVEDP was low throughout (2.5
Fig. 4. A: plots of SW versus LVEDP and TLVEDP during volumeloading in all animals and unloading (3 animals). Relations betweenSW and LVEDP all had a negative slope over at least part of thecurves. In all animals, there was a single positive SW-TLVEDPrelation during both volume loading and removal, suggesting thatpreload determined LV performance throughout volume manipula-tion and that there was no change in contractility. Right atrialpressure was used instead of PerP to estimate TLVEDP in dog 6. B:summary plot of the data from all the animals. Because PerP in dog2 (see Fig. 2) was much lower than RVEDP, RVEDP was usedinstead to calculate transmural LVEDP for this summary plot only. See Fig. 1 for abbreviations.
mmHg). Pericardial pressure was similar (Fig. 2, openand closed circles) over both ventricles in the threedogs in which both measurements were available. DISCUSSION
The most important findings of the present study are
as follows. First, change in LVEDP (or PCWP) is not areliable surrogate for estimating change in LVEDV in
Fig. 3. Plots of LVEDP and transmural LVEDP versus end-diastolic
severe congestive heart failure. Second, when trans-
segment length (SegL) during both volume loading in all animals
mural LVEDP was used to reflect LV distending pres-
(dogs 1–6) and unloading (3 animals). SegL was more closely relatedto transmural LVEDP than LVEDP.
sure, the negative slope of the SW-PCWP (apparent
AJP-Heart Circ Physiol • VOL 281 • DECEMBER 2001 • www.ajpheart.org
observed changes, the mechanism being similar to thatwhich was previously described in pulmonary embo-lism and chronic pulmonary disease (4, 5, 17). Commonto the three conditions is the presence of both pulmo-nary hypertension and constraint to LV filling. LVEDP-LVEDV relation and LV function. According
to Starling’s Law, SW increases as end-diastolic fiberlength or volume increases. Because volume is difficultto measure, LVEDP (or PCWP) is widely used as itssurrogate. This is based on the premise that LVEDVchanges in the same direction as LVEDP and that, atevery LVEDV, there is one value of LVEDP. SW shouldtherefore change in the same direction as LVEDP pro-vided there is no change in contractility or the amountof mitral regurgitation. This is normally a reasonableapproximation. In severe congestive heart failure, SWmay decrease as LVEDP increases; this “descendinglimb” of the Starling curve has therefore been attrib-uted to decreased contractility, each observation on thedescending limb representing different, progressivelydownward-displaced ventricular function curves (16,18). However, this interpretation presupposes thatLVEDP is the effective distending pressure and that
Fig. 5. Plots of SW versus SegL during volume loading in all animals
changes in LVEDP reflect changes in LVEDV. As ob-
and unloading in 3 animals. In 3 dogs, there is a positive slope of therelation and in 2, there was too little change in one or the other
served by Katz in 1955 (19), intracavitary and trans-
mural LVEDP are equal only when the pressure sur-rounding the LV is negligible. When the pressuresurrounding the LV is not negligible, external pressure
descending limb of the Starling curve, which implies
must be subtracted from LVEDP to calculate transmu-
decreased contractility) was eliminated. Thus contrac-
ral LVEDP accurately (the effective distending pres-
tility was not altered by volume manipulation in this
sure), which determines diastolic fiber length. Thus, if
model of congestive heart failure. This is the first
volume loading increases pressure around the LV more
demonstration of the potential effect of constraint to
than it increases intracavitary LVEDP, transmural
LV filling and ventricular interaction during volume
LVEDP will decrease (22). This will result in a de-
loading in congestive heart failure. Although our pre-
creased LVEDV and therefore, reduced SW in accor-
vious clinical study (26) had suggested that ventricular
dance with the Frank-Starling mechanism.
interaction might explain the previously observed as-
We demonstrated these principles previously in a
sociation of improved cardiac function when filling
pulmonary embolism model in which volume loading
pressure was reduced, it has not been previously veri-
shifted the LVEDP-LVEDV relation upward and left-
fied with simultaneous pressure and dimension mea-
ward, suggesting decreased compliance, and the SW-
LVEDP relation downward and rightward, suggesting
decreased contractility (4, 5). These apparent changes
LVEDP, which determines LVEDV) is equal to mea-
in compliance and contractility were eliminated when
sured LVEDP minus the surrounding pressure. We
transmural LVEDP was substituted for LVEDP: com-
have shown that intracavitary and transmural LVEDP
pliance and contractility remained unchanged. Jardin
may even change in opposite directions in acute pul-
et al. (17) demonstrated similar ventricular interaction
monary embolism (5). The results from the present
during volume loading in patients with chronic pulmo-
study show that the same phenomena may also occur
nary disease. The observation by Dupuis et al. (9) that
in congestive heart failure. Thus, although the nega-
SW increased as PCWP was reduced by nitroglycerin
tive slope of the SW-LVEDP relations at high LVEDPs
in some of their patients with heart failure can be
suggested that contractility decreased with volume
explained by the same mechanism, but this was not
loading, when transmural LVEDP was plotted instead,
addressed in their report. Whereas one might attribute
the apparent decrease in contractility was no longer
the improved SW to decreased systemic vascular resis-
evident. Indeed, there was a positive SW-transmural
tance and/or mitral regurgitation (10), that would not
LVEDP relation, indicating that systolic performance
account for the associated increase in LVEDV in these
was reliably predicted by the effective filling pressure,
patients. We recently demonstrated that lower body
consistent with Starling’s Law. The SW-segment
negative pressure (which decreases LVEDP) reduced
length relations provide additional support for the sug-
right atrial pressure and increased LVEDV in almost
gestion that contractility is not decreased during vol-
half of our study patients with severe heart failure (3).
ume loading. Our results also demonstrate that ven-
In the present study, we have now demonstrated that
tricular interaction contributes importantly to the
ventricular interaction explains the apparent paradox-
AJP-Heart Circ Physiol • VOL 281 • DECEMBER 2001 • www.ajpheart.org
ical responses in SW to volume manipulation in con-
and decrease LVEDV. This occurred during volume
gestive heart failure; the SW-LVEDP relation implied
loading in the present study; the transseptal pressure
that a descending limb of the Starling curve was
gradient decreased, RV diameter increased, and sep-
present, but ventricular performance was faithfully
tum-to-LV free wall diameter decreased.
predicted by the changes in transmural LVEDP. The
Implications. Our results suggest that the use of
SW-segment length relations provide additional sup-
LVEDP (or PCWP) to estimate changes in LV preload
port for our position that there is no descending limb of
in congestive heart failure may be quite misleading,
the curve, at least in this model of congestive failure.
particularly because the two may even change in op-
Pericardial pressure in congestive heart failure. Vol-
posite directions. The presence of increased jugular
ume loading normally increases LVEDV substantially
venous pressure suggests that pericardial pressure is
only until LVEDP reaches ϳ10–15 mmHg, after which
increased and therefore should alert the clinician to
the LVEDP-LVEDV relation becomes much steeper
the possibility that changes in PCWP may not reliably
because the pericardium limits further increases in
predict changes in LVEDV and, therefore, perfor-
cardiac volume (12, 24). Clearly, the pericardium can
mance. In fact, function may improve as PCWP is
grow in a time-dependent manner, as reported by
reduced (28), and the present study clarifies the mech-
LeWinter and Pavelec (21), who showed that con-
anism by which this can occur. To optimize benefit
straint became negligible several weeks after creation
from volume manipulation, transmural LVEDP or
of an arteriovenous shunt. Because the RV is thinwalled, transmural RVEDP is low, and as RVEDP
LVEDV should be assessed. Because of the close rela-
increases above 2–4 mmHg, pericardial pressure in-
tion between changes in right atrial and pericardial
creases in a parallel fashion (1). The thicker LV has a
pressures (7, 30), PCWP minus right atrial pressure
higher transmural pressure. In patients with and with-
might provide a reasonable estimate of transmural
out LV disease, ϳ30–40% of measured LVEDP is due
LVEDP, but this would have to be validated in clinical
to external constraint (8). In the present study, volume
studies. Because improved LV performance is the goal
loading increased the contribution of external pressure
of therapy, perhaps measuring cardiac output directly
to the measured LVEDP from ϳ50 to 80%.
is a better strategy. However, it is most important to
We recently reported that pericardial pressure var-
understand the potential for diastolic constraint and
ied widely among animals in the rapid-pacing model of
ventricular interaction and that changes in filling pres-
congestive failure (14) as it did in the present study. Of
sure alone should not be relied upon to predict re-
greater importance and in keeping with previous re-
ports, changes in RVEDP paralleled those in pericar-
Limitations. Our model does not completely mimic
dial pressure in both studies (4, 5, 25–27). Because
chronic severe congestive heart failure. Failure was of
there was no change in transmural RVEDP, we spec-
relatively short duration, and pulmonary artery pres-
ulate that when central venous pressure is acutely
sure was lower than is commonly observed in severe
increased, this implies increased pericardial con-
failure. We therefore speculate that there is potential
straint, a situation in which changes in filling pressure
for even greater ventricular interaction (and therefore,
may not accurately reflect changes in LVEDV. This is
“paradoxical” response to volume manipulation) in se-
consistent with studies in chronically instrumented
vere heart failure than was observed in the present
normal dogs and patients with heart failure; volume
study. That this may be true is suggested by much
loading increased LVEDV and SV only up to LVEDPs
greater increases in SW observed during tailored ther-
of 10–12 mmHg (6, 23, 31), after which there was no
apy in patients than in the present study (28).
further increase or even a decrease in SV (6).
Another potential limitation was the presence of a
Ventricular interaction. Whereas changes in trans-
variable amount of pericardial fluid that was drained
mural LVEDP explain the observed changes in SW
during instrumentation. This probably resulted in
during volume manipulation, consideration of the as-
some slackness of the pericardium and might have
minimized pericardial constraint and therefore, ven-
changes provides additional insight into the mecha-
tricular interaction. Reproducibility between experi-
nisms involved. Because the ventricles share the sep-tum and are surrounded by the poorly distensible peri-
ments might have been even better if it had been
cardium, in the presence of pericardial constraint, the
possible to control for this factor.
volume of one ventricle can increase substantially only
In conclusion, we have demonstrated substantial ex-
if the volume of the other decreases. The transseptal
ternal constraint in this model of pacing-induced con-
pressure gradient determines end-diastolic septal po-
gestive heart failure. The observed changes in LV per-
sition; changes in the transseptal pressure gradient
formance during volume manipulation were fully
shift the septum and, in the presence of constraint, can
explained by changes in the effective distending pres-
cause reciprocal changes in the volumes of the ventri-
sure and Starling’s Law when preload was appropri-
cles. In the presence of pulmonary hypertension, vol-
ately assessed. These results underscore the need to
ume loading is likely to increase RVEDP more than
consider the potential effects of pericardial constraint
LVEDP (5, 17). If this occurs, the resulting decrease in
and ventricular interaction on LV filling when assess-
the transseptal pressure gradient will shift the septum
ing the effects of therapy on cardiac function in heart
leftward (4, 20) thereby tending to increase RVEDV
AJP-Heart Circ Physiol • VOL 281 • DECEMBER 2001 • www.ajpheart.org
This study was supported in part by grants-in-aid from the Al-
16. Howarth S, McMichael J, and Sharpey-Schafer EP. Effects
berta Heart and Stroke Foundation (Calgary) held by I. Belenkie and
of venesection in low output heart failure. Clin Sci (Colch) 6:
by J. V. Tyberg and by grants from the British Heart Foundation (to
M. P. Frenneaux, J. A. Morris-Thurgood, and T. D. Moore).
17. Jardin F, Gueret P, Prost JF, Farcot JC, Ozier Y, and Bourdarias JP. Two-dimensional echocardiographic assess- REFERENCES
ment of left ventricular function in chronic obstructive pulmo-nary disease. Am Rev Respir Dis 129: 135–142, 1984.
1. Applegate RJ, Johnston WE, Vinten-Johansen J, Klopfen-
18. Katz AM. The descending limb of the Starling curve and the stein HS, and Little WC. Restraining effect of intact pericar-
failing heart. Circulation 32: 871–875, 1965.
dium during acute volume loading. Am J Physiol Heart Circ
19. Katz LN. Analysis of the several factors regulating the perfor- Physiol 262: H1725–H1733, 1992.
mance of the heart. Physiol Rev 35: 91–106, 1955.
2. Armstrong PW, Stopps TP, Ford SE, and DeBold AJ. Rapid
20. Kingma I, Tyberg JV, and Smith ER. Effects of diastolic
ventricular pacing in the dog: pathophysiologic studies of heart
transseptal pressure gradient on ventricular septal position and
failure. Circulation 74: 1075–1084, 1986.
motion. Circulation 68: 1304–1314, 1983.
3. Atherton JJ, Moore TD, Lele SS, Thomson HL, Galbraith
21. LeWinter MM and Pavelec R. Influence of the pericardium on AJ, Belenkie I, Tyberg JV, and Frenneaux MP. Diastolic
left ventricular end-diastolic pressure-segment relations during
ventricular interaction in chronic heart failure. Lancet 349:
early and later stages of experimental chronic volume overload
in dogs. Circ Res 50: 501–509, 1982.
4. Belenkie I, Dani R, Smith ER, and Tyberg JV. Ventricular
22. Mirsky I and Rankin JS. The effects of geometry, elasticity,
interaction during experimental acute pulmonary embolism.
and external pressures on the diastolic pressure-volume and
Circulation 78: 761–768, 1988.
stiffness-stress relations. How important is the pericardium?
5. Belenkie I, Dani R, Smith ER, and Tyberg JV. Effects of Circ Res 44: 601–611, 1979.
volume loading during experimental acute pulmonary embolism.
23. Parker JO and Case RB. Normal left ventricular function. Circulation 80: 178–188, 1989. Circulation 60: 4–12, 1979.
6. Boettcher DH, Vatner SF, Heyndrickx GR, and Braun-
24. Rabkin SW and Hsu PH. Mathematical and mechanical mod- wald E. Extent of utilization of the Frank-Starling mechanism
eling of stress-strain relationship of pericardium. Am J Physiol
in conscious dogs. Am J Physiol Heart Circ Physiol 234: H338–
25. Smiseth OA, Refsum H, and Tyberg JV. Pericardial pressure
7. Boltwood CM, Skulsky A, Drinkwater DC, Lang S, Mulder
assessed by right atrial pressure: a basis for calculation of left
DG, and Shah PM. Intraoperative measurement of pericardial
ventricular transmural pressure. Am Heart J 108: 603–605,
constraint: role in ventricular diastolic mechanics. J Am CollCardiol 8: 1289–1297, 1986.
26. Smiseth OA, Thompson CR, Ling H, Robinson M, and
8. Dauterman K, Pak PH, Maughan WL, Nussbacher A, Arieˆ Miyagishima RT. Juxtacardiac pleural pressure during posi- S, Liu CP, and Kass DA. Contribution of external forces to left
tive end-expiratory pressure ventilation: an intraoperative study
ventricular diastolic pressure. Implications for the clinical use of
in patients with open pericardium. J Am Coll Cardiol 23: 753–
the Starling law. Ann Intern Med 122: 737–742, 1995.
9. Dupuis J, LaLonde G, Lebeau R, Bichet D, and Rouleau
27. Smiseth OA, Thompson CR, Ling H, Robinson M, and JL. Sustained beneficial effect of a seventy-two hour intravenous Miyagishima RT. A potential clinical method for calculating
infusion of nitroglycerin in patients with severe chronic conges-
transmural left ventricular filling pressure during positive end-
tive heart failure. Am Heart J 120: 625–637, 1990.
expiratory pressure ventilation: an intraoperative study in hu-
10. Faggiono P, Rusconi C, and Ghizzoni G. Nitrates in heart
mans. J Am Coll Cardiol 27: 155–160, 1996.
failure: the hemodynamic effects and clinical implications. Car-
28. Stevenson LW and Tillisch JH. Maintenance of cardiac out-
put with normal filling pressures in patients with dilated heart
11. Farrar DJ, Chow E, and Brown CD. Isolated systolic and
failure. Circulation 74: 1303–1308, 1986.
diastolic ventricular interactions in pacing-induced dilated car-
29. Suzuki M, Cheng CP, Ohte N, and Little WC. Left ventric-
diomyopathy and effects of volume loading and pericardium.
ular spherical dilation and regional contractile dysfunction in
Circulation 92: 1284–1290, 1995.
dogs with heart failure. Am J Physiol Heart Circ Physiol 273:
12. Flessas AP and Ryan TJ. Left ventricular diastolic capacity in
man. Circulation 65: 1197–1203, 1982.
30. Tyberg JV, Taichman GC, Smith ER, Douglas NWS, Smis-
13. Hamilton DR, DeVries G, and Tyberg JV. Static and dy- eth OA, and Keon WJ. The relation between pericardial pres-
namic operating characteristics of a pericardial balloon. J Appl
sure and right atrial pressure: An intraoperative study. Circu-
14. Horne SG, Belenkie I, Tyberg JV, and Smith ER. Pericar-
31. Vatner SF and Boettcher DH. Regulation of cardiac output by
dial pressure in experimental heart failure. Can J Cardiol 16:
stroke volume and heart rate in conscious dogs. Circ Res 42:
15. Howard RJ, Stopps TP, Moe GW, Gotlieb A, and Arm-
32. Wilson JR, Douglas P, Hickey WF, Lanoce V, Ferraro N, strong PW. Recovery from heart failure: structural and func- Muhammad A, and Reichek N. Experimental congestive
tional analysis in a canine model. Can J Physiol Pharmacol 66:
heart failure produced by rapid ventricular pacing in the dog:
cardiac effects. Circulation 75: 857–867, 1987. AJP-Heart Circ Physiol • VOL 281 • DECEMBER 2001 • www.ajpheart.org
 Ventricular interaction and external constraint accountfor decreased stroke work during volume loading in CHF
THOMAS D. MOORE,1 MICHAEL P. FRENNEAUX,1 ROZSA SAS,2J. J. ATHERTON,3 JAYNE A. MORRIS-THURGOOD,1 ELDON R. SMITH,2JOHN V. TYBERG,2 AND ISRAEL BELENKIE22Departments of Medicine and Physiology and Biophysics, University of Calgary,Calgary, Alberta T2N 4N1, Canada; 3University of Queensland, Brisbane Q4029, Australia;and 1Department of Cardiology, Wales Heart Research Institute,University of Wales College of Medicine, Cardiff CF14 4XN, United Kingdom
Received 26 April 2001; accepted in final form 13 August 2001
Moore, Thomas D., Michael P. Frenneaux, Rozsa Sas,
Ventricular interaction and external constraint accountfor decreased stroke work during volume loading in CHF
THOMAS D. MOORE,1 MICHAEL P. FRENNEAUX,1 ROZSA SAS,2J. J. ATHERTON,3 JAYNE A. MORRIS-THURGOOD,1 ELDON R. SMITH,2JOHN V. TYBERG,2 AND ISRAEL BELENKIE22Departments of Medicine and Physiology and Biophysics, University of Calgary,Calgary, Alberta T2N 4N1, Canada; 3University of Queensland, Brisbane Q4029, Australia;and 1Department of Cardiology, Wales Heart Research Institute,University of Wales College of Medicine, Cardiff CF14 4XN, United Kingdom
Received 26 April 2001; accepted in final form 13 August 2001
Moore, Thomas D., Michael P. Frenneaux, Rozsa Sas,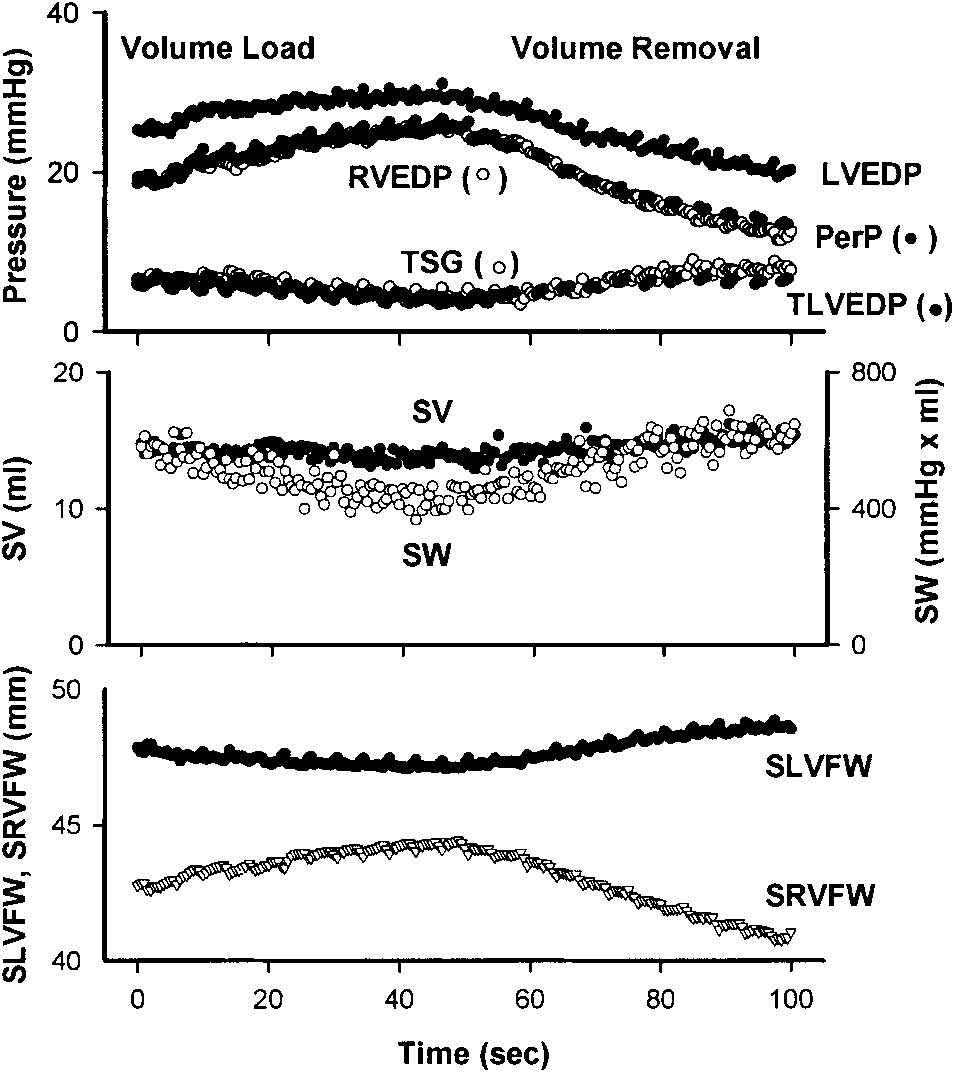
 ulation. Figure 1 illustrates the changes in pressures,LV performance, and dimensions during volume load-ing and removal in a representative dog (dog 5). Vol-ume loading increased LVEDP (from 20.9 Ϯ 1.8 to26.8 Ϯ 2.9 mmHg) but increased RVEDP more (from15.1 Ϯ 1.6 to 24.3 Ϯ 2.3 mmHg), thus decreasing thetransseptal pressure gradient (from 6.4 Ϯ 1.1 to 3.0 Ϯ1.1 mmHg). As shown in Fig. 2, the increase in peri-cardial pressure during volume loading (from 13.6 Ϯ1.9 to 21.8 Ϯ 3.2 mmHg) was similar to the increase inRVEDP. The decrease in transmural LVEDP (from6.6 Ϯ 0.7 to 4.5 Ϯ 1.1 mmHg) was similar to thedecrease in the transseptal pressure gradient. Thedecreased transseptal pressure gradient and transmu-ral LVEDP were associated with a decreased SV (from11.7 Ϯ 2.8 to 10.1 Ϯ 2.6 ml) and SW (from 418 Ϯ 101 to291 Ϯ 78 ml ⅐ mmHg). All of the above changes werestatistically significant. The changes in peak LV sys-tolic pressure, peak RV systolic pressure, and heartrate were not significant.
ulation. Figure 1 illustrates the changes in pressures,LV performance, and dimensions during volume load-ing and removal in a representative dog (dog 5). Vol-ume loading increased LVEDP (from 20.9 Ϯ 1.8 to26.8 Ϯ 2.9 mmHg) but increased RVEDP more (from15.1 Ϯ 1.6 to 24.3 Ϯ 2.3 mmHg), thus decreasing thetransseptal pressure gradient (from 6.4 Ϯ 1.1 to 3.0 Ϯ1.1 mmHg). As shown in Fig. 2, the increase in peri-cardial pressure during volume loading (from 13.6 Ϯ1.9 to 21.8 Ϯ 3.2 mmHg) was similar to the increase inRVEDP. The decrease in transmural LVEDP (from6.6 Ϯ 0.7 to 4.5 Ϯ 1.1 mmHg) was similar to thedecrease in the transseptal pressure gradient. Thedecreased transseptal pressure gradient and transmu-ral LVEDP were associated with a decreased SV (from11.7 Ϯ 2.8 to 10.1 Ϯ 2.6 ml) and SW (from 418 Ϯ 101 to291 Ϯ 78 ml ⅐ mmHg). All of the above changes werestatistically significant. The changes in peak LV sys-tolic pressure, peak RV systolic pressure, and heartrate were not significant.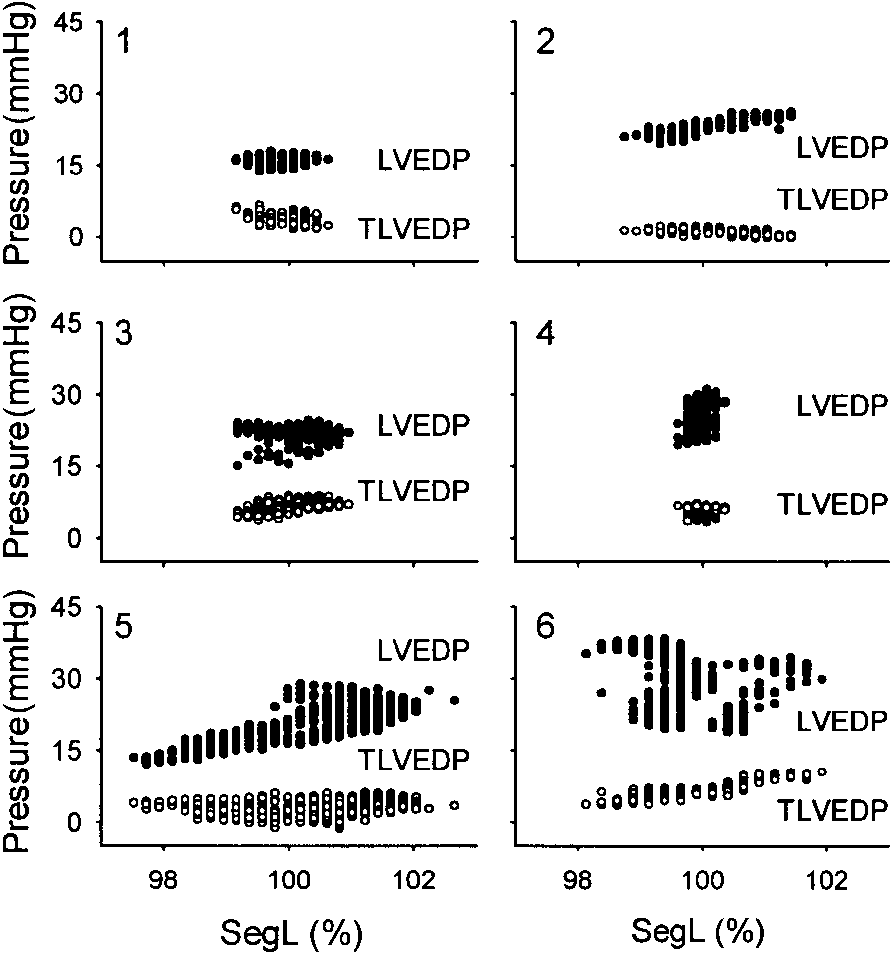
 LV segment length. Figure 3 shows the LVEDP- and
transmural LVEDP-segment length relations in eachanimal. As can be seen, transmural LVEDP was con-sistently lower than LVEDP and segment length wasmore closely related to transmural LVEDP thanLVEDP. There was little change in segment length indog 4, and there was little change in pressure in dog 1.
LV segment length. Figure 3 shows the LVEDP- and
transmural LVEDP-segment length relations in eachanimal. As can be seen, transmural LVEDP was con-sistently lower than LVEDP and segment length wasmore closely related to transmural LVEDP thanLVEDP. There was little change in segment length indog 4, and there was little change in pressure in dog 1.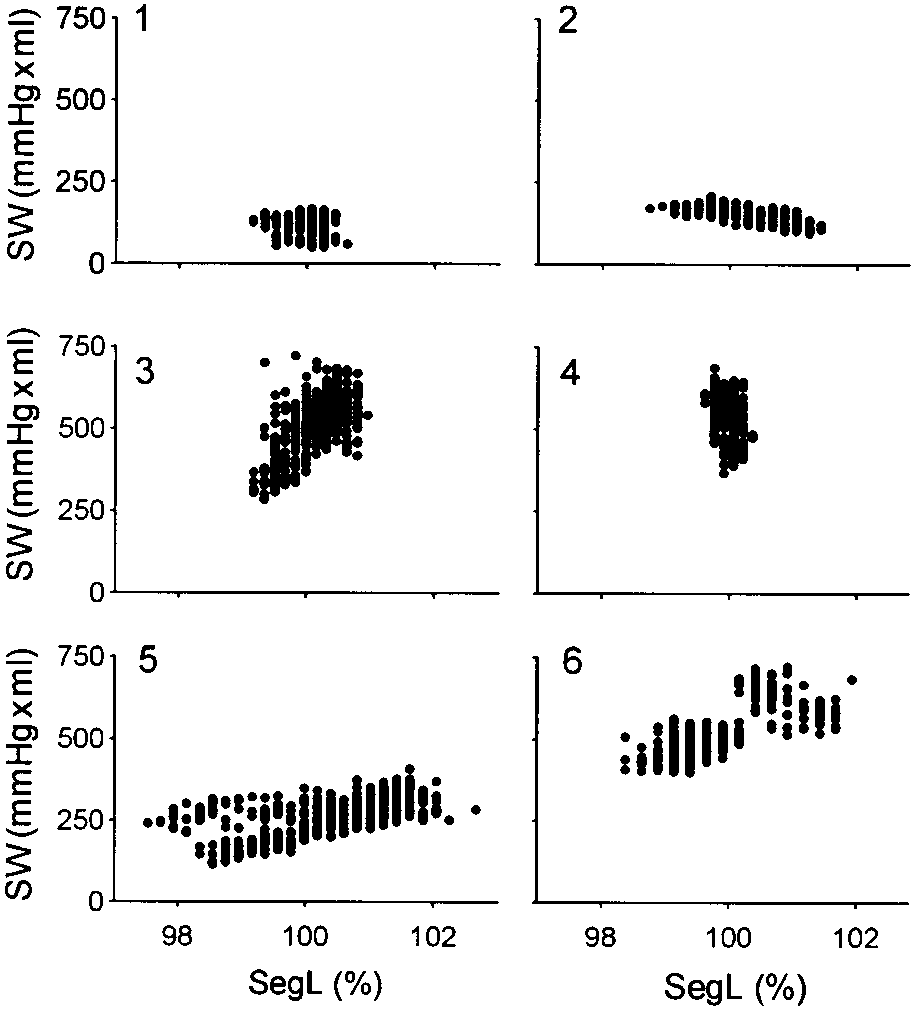 observed changes, the mechanism being similar to thatwhich was previously described in pulmonary embo-lism and chronic pulmonary disease (4, 5, 17). Commonto the three conditions is the presence of both pulmo-nary hypertension and constraint to LV filling.
observed changes, the mechanism being similar to thatwhich was previously described in pulmonary embo-lism and chronic pulmonary disease (4, 5, 17). Commonto the three conditions is the presence of both pulmo-nary hypertension and constraint to LV filling.