Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Anesthesia.ucsd.edu
Intensive Care Med (2004) 30:444–449DOI 10.1007/s00134-003-2117-0
Olanzapine vs haloperidol: treating delirium
UniversitØ de MontrØal),Montreal, Quebec, Canada
ments: Patient’s delirium severity andbenzodiazepine use were monitored
Division of Respiratory and Critical Care,
McGill University Health Centre,Montreal, Quebec, Canada
Published recommendations for delirium treatment in
the ICU are empiric. Antipsychotic administration is
Delirium in the intensive care unit (ICU) setting has
broadly accepted, especially for agitated delirium [11].
generated interest recently. Its occurrence is associated
The use of antipsychotics is based on the belief that such
with adverse outcomes: self-extubation, removal of
intervention will shorten symptom severity and duration
indwelling catheters [1], prolonged ventilator dependence
[12]. Haloperidol is the medication most commonly used
[2], and lengthened ICU and hospital stay [3, 4, 5].
in critical care practice. Intravenous administration pre-
Delirium is not associated with increased ICU mortality
sumes that this route is more effective in emergency
[1, 2] but seems an independent marker for increased 1-
situations, with less extrapyramidal side effects [13]. This
year mortality [6]. Recognizing delirium remains chal-
approach, with rapid dose escalation, is specifically
lenging [7, 8]. Recent tools have been developed to screen
recommended in textbooks [14] and recently published
for [9] and aid in identification of [10] delirium in the
ICU. Clinical management and pharmacologic treatment
Despite its broad acceptance in clinical practice,
haloperidol is not without adverse effects. Cognitive
“numbness” and dysphoria are well recognized and occur
as agreement from the attending physician were obtained prior to
in 40% of studied subjects [16]. Extrapyramidal side
effects, such as akathisia and oropharyngeal dysfunction,have been described [16, 17]. Neuroleptic malignant
syndrome and dystonic reactions, including laryngospasmand trismus, are also reported [18, 19].
After randomization on an even/odd day basis for haloperidol or
Haloperidol causes ventricular arrhythmias, torsades
olanzapine, the intensivist prescribed the antipsychotic orally or viaenteral tube within 2 h of the diagnosis of delirium. Haloperidol
de pointe, and cardiac arrest, especially in patients with
was initiated at 2.5–5 mg every 8 h, and olanzapine was begun at
cardiac disease both with and without preceding QT
5 mg daily. Patients over 60 years received a lower initial dosage
interval prolongation [20]. QT prolongation has been
(haloperidol 0.5–1 mg, or olanzapine 2.5 mg). Subsequent titration
reported with low-dose haloperidol. Finally, some pa-
was based on clinical judgment. All administered doses ofmedication were recorded. We noted the use of benzodiazepines
tients may be resistant to haloperidol. All patients thus
as adjuvant treatment. Clinicians and nurses titrated sedative
require ongoing assessment of its therapeutic effect [21].
dosage with the Ramsay scale. Intravenous haloperidol adminis-
The severity of comorbid conditions commonly ob-
tration was left to the treating intensivist’s discretion.
served in the ICU raises concerns about haloperidol’spotential adverse effects. In some patients haloperidol is
clearly contraindicated. An alternative medication whichoffers symptomatic control of delirium with less frequent
Demographic information, type of admission, and Acute Physiol-
and less severe adverse effects would be clinically useful
ogy and Chronic Health Evaluation (APACHE II) scores were
in the delirious ICU patient. New second-generation
collected when delirium was diagnosed. Objective evaluations wereperformed on a daily basis by a clinician or research nurse blinded
antipsychotics with more favorable pharmacologic pro-
to the dispensed medication. The measures obtained at baseline and
files have been introduced for the treatment of schizo-
daily up to a maximum of 5 days in the ICU were:
phrenia. Their potential benefit in delirium treatment hasrecently been explored [22, 23, 24, 25, 26]; one of these,
1. Vital signs. 2. Liver function tests.
olanzapine, has a reported oral bioavailability of 80% and
3. Daily dose of antipsychotic study medication.
Because of early encouraging reports [22, 23, 24, 25,
5. Daily dose of sedatives if used specifically for sedation.
26], we conducted a prospective randomized controlled
Benzodiazepines doses were converted to lorazepam equiva-lents [29].
trial to evaluate the safety and clinical utility of one such
6. Daily dose of antiparkinsonian medication prescribed for
agent, olanzapine, as an alternative to haloperidol for
treatment of delirium in the intensive care setting.
7. Delirium index (DI), as previously described [30], administered
by one of three individuals (two research nurses, one physician)trained its use. This delirium severity scale is based on sevenitems associated with delirium, each rated on a four-point scale
for a maximum score of 21. The evaluator was blinded to thepatient’s treatment.
8. Daily worst Ramsay score [31] obtained at least once every 8-h
From July 2000 to September 2001, patients aged 18–75 years
9. Extrapyramidal signs assessed with Ross-Chouinard [32] and
admitted to a 16-bed medical-surgical ICU (Maisonneuve-Rose-
Angus-Simpson scales [33] by a physician.
mont Hospital, Montreal,) for more than 24 h were screened threetimes daily for delirium utilizing the ICU Delirium ScreeningChecklist, ICU-DSC, as previously described [9]. In screened
patients with an ICU DSC of !4 or with clinical manifestationsdelirium, the diagnosis was confirmed by a physician using DSM-
Comparisons of medical and demographic characteristics were
IV criteria [28]. All patients with delirium were considered eligible
performed with Fisher’s exact test and Student’s t test. Analysis of
variance for repeated measures was used for group comparisons on
Pregnant patients, those who received antipsychotic medication
the DI severity scores, and total daily benzodiazepine dose, based
within 10 days prior to hospital or ICU admission, or in whom
on a 25 mixed model, (i.e., two groups measured at five time
either haloperidol or olanzapine was contraindicated were exclud-
points). When indicated, Greenhouse-Geisser correction was
ed. Contraindications to drug administration were Parkinson’s
applied to adjust for unstable between-measures correlation. All
disease, oropharyngeal dysfunction, prolonged QT interval, and
simple main effects were calculated, in order to assess group
differences at each time point and study patterns of change within
Individuals with gastrointestinal dysfunction, precluding oral/
each of the two groups. Sidaks multiple comparisons procedure was
enteral drug administration, or whose neurological status did not
used for post-hoc time-point comparisons.
permit an adequate neuropsychiatric evaluation (e.g., stupor or
Inter-rater reliability was evaluated with the intra-class corre-
coma), were also excluded from the study. Patients who developed
lation coefficient, using a two-way random-effects model. Since
agitation during the study were permitted intravenous haloperidol
delirium is a fluctuating disorder, intra-rater reliability was not
administration (recorded as “rescue haloperidol”).
The research protocol was approved by the institutional
scientific and ethics committee. Written informed consent as well
Of 1009 patients admitted to the ICU during the studyperiod, 214 patients were diagnosed with delirium. Ofthose, 103 were considered eligible for the study (exclu-sions were due primarily to gastrointestinal dysfunction). Informed consent was obtained in 80 patients; of these,the treating physician withdrew 3 patients, status changedto “no active treatment” in 2, drug interaction wassuspected in 1, and data was lost in 1 patient. Seventy-three patients were included in the final analysis. Sixty-one patients remained alive and in the hospital for 3 daysor more, accounting for the difference between therandomized and 3-day analysis. Patient characteristicsare shown in Table 1. Gender distribution (p=0.43) andAPACHE II scores (p=0.14) were comparable, as werepatient weights (p=0.9). The study population waspredominantly surgical. The difference between the
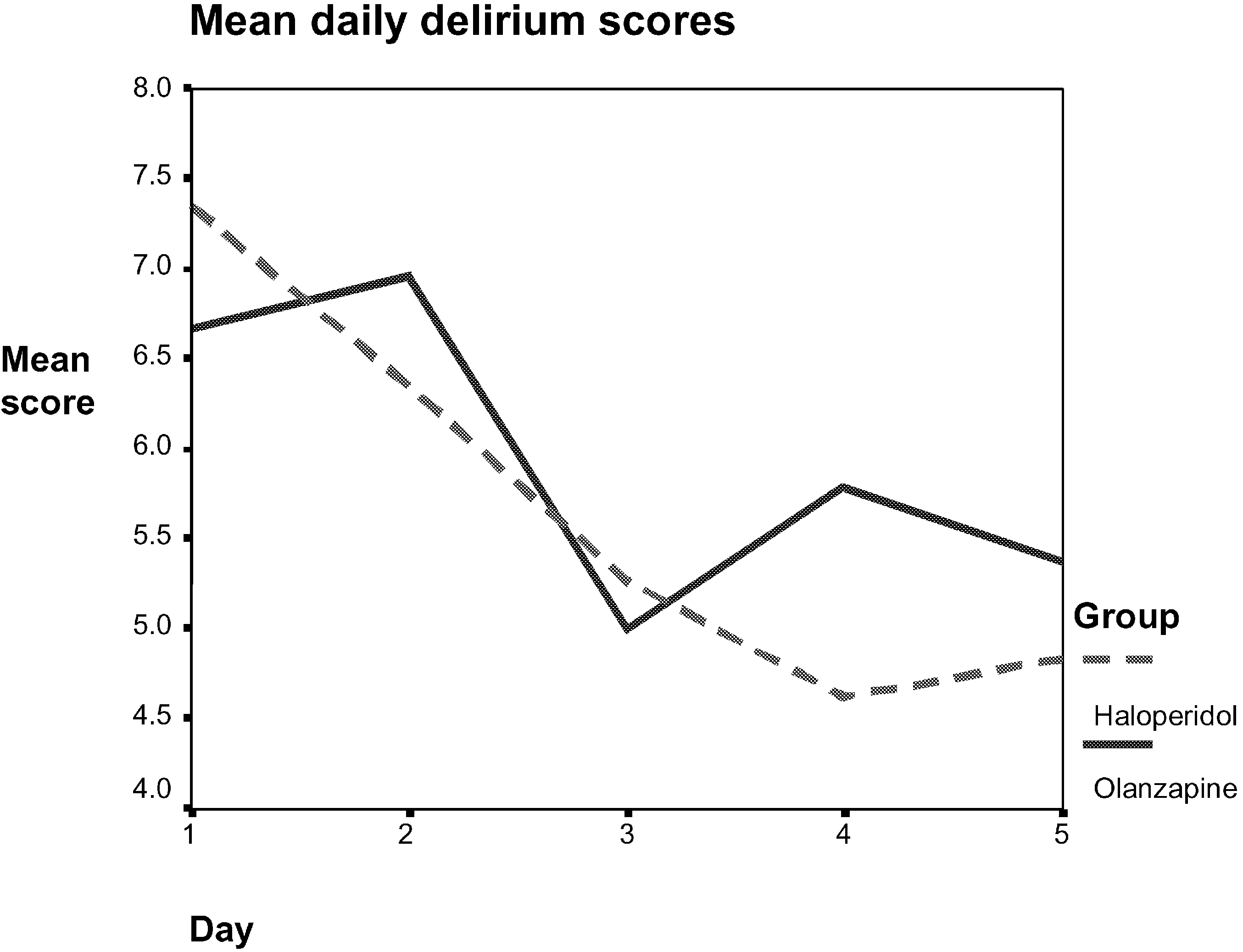
Fig. 1 Delirium index scores were performed daily and are shown
urgent/elective surgical patient ratio did not reach statis-
over time. Overall delirium indices decreased over time (7.08 for
tical significance (p=0.057). The mean age of patients
all patients on day 1 decreasing to 5.05 on day 5). There are no
receiving haloperidol (63.26€11.66 years) was lower
than the age of the group receiving olanzapine (67.50€6.04 years, p=0.046). Other clinical characteristics relatedto reasons for ICU admission, as well as co-morbidities,
were no different between the groups.
Patients in the haloperidol group received were given a
Figure 2 depicts the benzodiazepine dose requirements
mean enteral daily dose of 6.5 mg of drug (range 1–
over time, expressed in lorazepam equivalents [29]. The
28 mg) compared with 4.54 mg for the olanzapine group
square root of benzodiazepine doses was used to correct
(range 2.5–13.5 mg). Rescue intravenous haloperidol was
for non-normal distributions as well as the withdrawal of
used primarily on the first day (10 of 28 in the olanzapine
one subject (no. 64) from the analysis because benzodi-
group, range 1–5 mg, 2.32€1.32 mg; vs 19 of 45 in the
azepine values on days 4 and 5 were atypical (24 and
haloperidol group, range 1–5 mg, 2.92€1.56 mg). From
26 mg, respectively). Analysis of variance did not identify
day 2 onwards, 5 patients received rescue haloperidol in
any differences between the two groups, at any of the five
doses ranging from 1 to 3 mg. Only one olanzapine
measurement times (interaction effect p=0.94, group
patient required one rescue haloperidol dose on day 3.
effect p=0.9). There was, however, a time effect
The proportion of patients requiring intravenous haloper-
(p=0.02) reflecting the decrease in dosages required over
idol (p=0.63) and the amount of IV haloperidol required
in each group (Z=0.97, p=0.35) were similar.
The dose of rescue haloperidol, opiates, sedatives other
The results of the daily DI scores are summarized in
than benzodiazepines, Ramsay scores, vital signs, and
Fig. 1. A comparable reduction in DI was noted over time
liver function tests were no different between groups.
in both groups, with no difference between patients
Most patients received continuous infusions of fentanyl,
treated with haloperidol vs olanzapine (ANOVA time
the preferred opiate analgesic in our ICU, in doses
effect p=0.02, group effect p=0.83, interaction effect
ranging from 50 to 100 mg/h. Propofol was not used.
p=0.64). Inclusion of patients present for only 3 or 4 days
Ramsay scores ranged from 1 to 3 in both groups with the
did not modify the results. Overall agreement between
exception of the first 24 h, during which approximately a
admission, and acute physiolo-gy and chronic health evalua-
Intravenous (IV) administration of haloperidol has
gained acceptability in the ICU based on a single,unblinded, non-randomized study in which IV adminis-tration produced fewer extrapyramidal side effects (com-pared with enteral haloperidol) in 10 patients [13]. Although clinical experience and textbook recommenda-tions have resulted in the universal use of intravenoushaloperidol in this setting, few authors mention itsdrawbacks and potential for therapeutic failure [34, 35]. Enteral haloperidol was compared with olanzapine be-cause olanzapine was not available in parenteral form; wewished to exclude differences attributable to administra-tion route. Bioavailability of either drug may have beenslow as a result, although absorption or bioavailabilityshould have been similar for the two medications. This isindirectly supported by the fact that neither measures ofclinical outcomes nor the use of rescue or adjunctive
Fig. 2 Benzodiazepine mean daily dose doses were calculated per
medication differed between the two treatment arms.
24 h per patient and are shown over time. There are no differences
Despite unreliable systemic absorption of enteral medi-
cations in the critical care setting, correction of a “lowcholinergic excess dopaminergic state” (one of the
third of the patients, evenly distributed among the groups,
mechanisms by which antipsychotics are felt to affect
had mild agitation. Extrapyramidal symptoms were
delirium) may have occurred with relatively low dose of
carefully recorded. Among the patients receiving halo-
peridol, 6 rated low scores on extrapyramidal symptom
Intravenous rescue haloperidol, used in the first 24 h in
testing (1 for the Ross Chouinard, 1–4 for the Simpson-
both groups, may have contaminated the early DI
Angus scale). Patients on olanzapine had no extrapyra-
evaluation between the groups. Given the reported half-
midal manifestations. No patient in either group received
life of intravenous haloperidol, however, and the small
prophylactic or therapeutic antiparkinsonian therapy.
number of patients who required it beyond the first day, it
There were no adverse effects (specific or otherwise)
is unlikely the overall beneficial evolution of the olan-
zapine group over time is attributable to the rescuehaloperidol received on the first day.
The population studied included a greater proportion
of surgical than medical patients. Surgical vs medicaldisease is not recognized [1] as influencing the incidence
Management of delirium in ICU patients whose co-
morbidities render the physician reluctant to administer
Delirium subtypes [8, 37] were not explicitly described
haloperidol can be problematic. Recent studies have
because of previous work suggesting that “quiet,” non-
explored the safety and efficacy of novel antipsychotics in
agitated delirium is just as morbid as delirium accompa-
the management of delirium outside the ICU [22, 23, 24,
nied by agitation [1]. Independently, agitation in the ICU
may be ascribed to a number of factors other than
We compared enteral haloperidol and olanzapine, in
delirium. The ICU in which the study was performed has
consecutively admitted eligible ICU patients with delir-
a clinical expertise in delirium screening. This may
ium. The DI, a tool specifically designed to measure
account for the low delirium scores on diagnosis and
changes in the severity of the symptoms of delirium, was
throughout the study. No patients were identified with
chosen because it was easy to perform in an intensive care
severe initial psychomotor agitation and delirium requir-
setting (in contrast to the widely used Delirium Rating
ing immediate intravenous haloperidol administration
Scale or the Memorial Delirium Assessment Scale). Both
prior to study entry. Patients seldom reach this state in
olanzapine and haloperidol were effective in reducing
our unit, we believe, because of systematic screening for
delirium symptoms. The clinical course in both treatment
thought content as part of an ICU Delirium Screening
arms was unmarred by severe agitation. Olanzapine
Checklist [9] which is used routinely in all patients. The
patients had no adverse effects attributable to the drug,
relatively low daily dose of benzodiazepines utilized
whereas 6 patients receiving haloperidol developed
further support this hypothesis. Almost all patients also
received opiate analgesics, which may have decreased theoverall use of anxiolytics such as benzodiazepines.
This study’s main limitation is the uneven distribution
its use in ICU patients. Cardiac toxicity, including
between the two treatment groups. Drug allocation
arrhythmias and QT prolongation, have not been de-
sequences should ideally be completely random and
scribed with olanzapine. Olanzapine is costlier than
concealed. The odd/even day randomization, chosen for
haloperidol; however, in view of the comparable efficacy
convenience, was not corrected for the slightly more
in reducing delirium symptoms, olanzapine can perhaps
frequent occurrence of odd days on which patients were
be recommended for patients in whom cardiac disease,
randomized to receive haloperidol in this study. Although
QT prolongation, or other features preclude haloperidol
not explicit, the research nurse’s or physician’s random-
ization based on odd/even days may have inadvertently
This represents the first prospective randomized study
led to bias on their part, or on the part of the treating team
of antipsychotic treatment for delirium in an ICU. The
who may have guessed the randomization sequence. The
issue warrants further exploration in delirious ICU
treating physicians and nurses were not blinded to the
patients with higher APACHE scores. The availability
assigned drug. Reporting bias (with regard to the day
of olanzapine in parenteral form may broaden its appli-
delirium developed) may have influenced subsequent
cability. This preliminary work suggests olanzapine is
administration of the study or other medications.
safe and effective in reducing delirium symptoms.
Haloperidol and olanzapine dosages were within
ranges described for treating delirium in other settings[24, 25, 26]. The severity of delirium and the clinical
response suggested a 20–30% drop in DI ratings withsizeable standard deviation variability, precluding com-
In ICU delirium, olanzapine is a treatment alternative to
parative statements about the therapeutic effectiveness of
haloperidol. Its use could benefit patients with underlying
Parkinson’s disease, a prolonged QT interval, or oropha-
Olanzapine seems a safe alternative to haloperidol for
ryngeal dysfunction, which preclude the safe administra-
the treatment of acute delirium in ICU patients. Although
tion of haloperidol. Its recommendation as treatment for
the small sample size limits the statistical evaluation of
delirium in the critical care setting is limited by its current
side effects between groups, few adverse effects were
noted in either group. The absence of extrapyramidal sideeffects in the olanzapine group is in keeping with the
Acknowledgement Support for this study was generously provided
findings described by Breitbart et al. [26], and in favor of
by a (peer-reviewed) grant from the Zyprexa fund, Eli-Lilly, NorthAmerica.
delirium in the intensive care unit. Clin
15. Jacobi J, Fraser GL, Coursin DB, Riker
intensive care unit on hospital length of
practice guidelines for the sustained use
ically ill adult. Crit Care Med 30:119–
ium predicts 12-month mortality. ArchIntern Med 162:457–463
Antipsychotic drug-induced dysphoria.
Olanzapine in the treatment of delirium.
dysphagia and aspiration: a brief report.
for delirium in the Korean population.
the treatment of delirium in hospitalized
34. Skrobik Y (2002) Haloperidol should be
peridol after coronary bypass surgery.
37. Ross CA, Peyser CE, Shapiro I, Folstein
of risperidone in delirium: case reports.
risperidone. Int J Geriatr Psychophar-macol 1:24–26
European Journal of Clinical Nutrition (2013) 67, 71–74& 2013 Macmillan Publishers LimitedEffect of daily consumption of probiotic yoghurt on insulinresistance in pregnant women: a randomized controlled trialZ Asemi1, M Samimi2, Z Tabassi2, M Naghibi Rad1, A Rahimi Foroushani3, H Khorammian1 and A Esmaillzadeh4,5BACKGROUND/OBJECTIVES: Owing to excess body weight and increased secretion of
Diabetes La diabetes generalmente es una enfermedad de por vida (crónica) en la cual hay niveles altos de La insulina es una hormona producida por el páncreas para controlar el azúcar en la sangre. La diabetes puede ser causada por muy poca producción de insulina, resistencia a ésta o ambas. Para comprender la diabetes, es importante entender primero el proceso normal por medio del cua
 Of 1009 patients admitted to the ICU during the studyperiod, 214 patients were diagnosed with delirium. Ofthose, 103 were considered eligible for the study (exclu-sions were due primarily to gastrointestinal dysfunction).
Of 1009 patients admitted to the ICU during the studyperiod, 214 patients were diagnosed with delirium. Ofthose, 103 were considered eligible for the study (exclu-sions were due primarily to gastrointestinal dysfunction).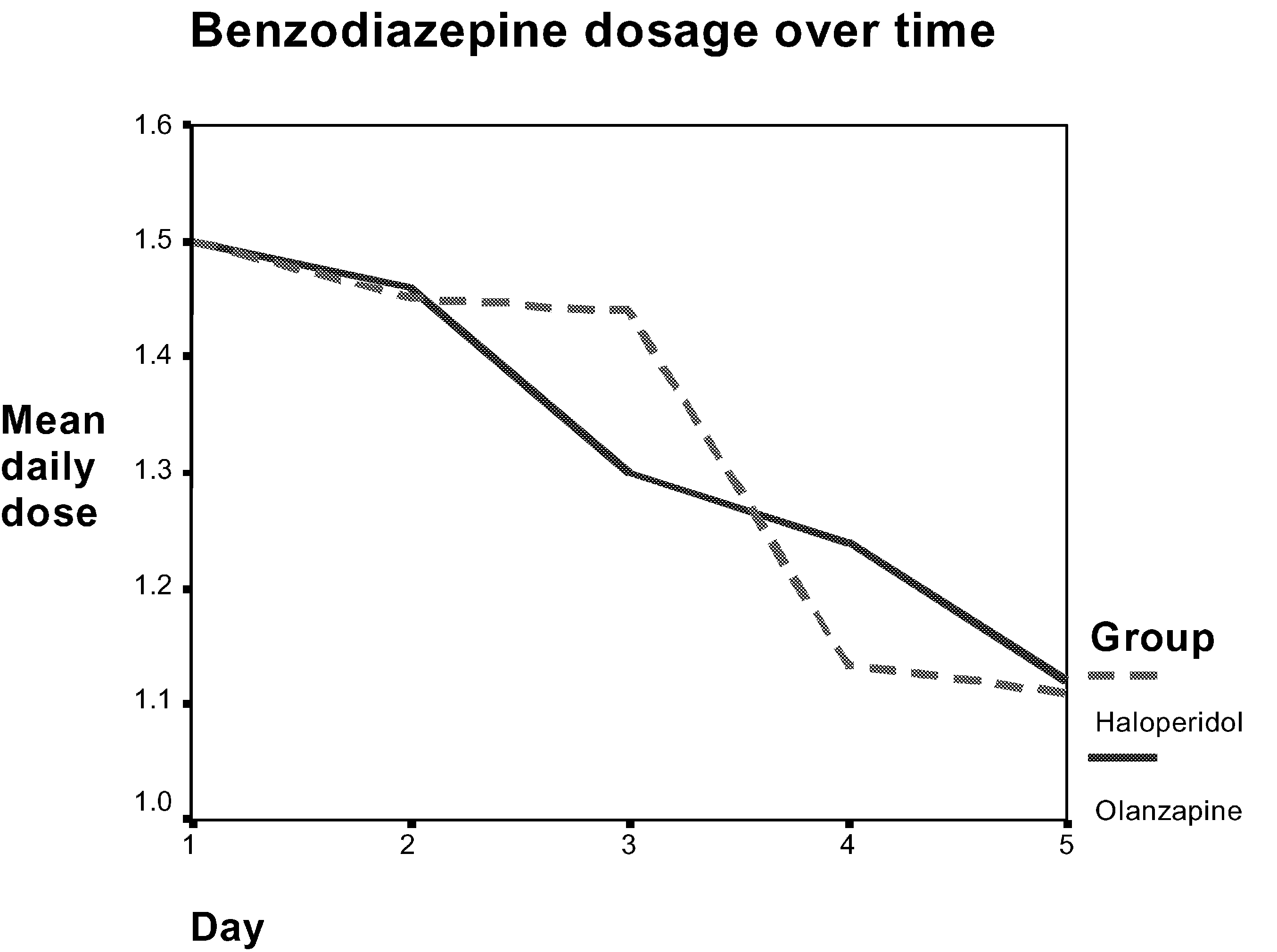 Intravenous (IV) administration of haloperidol has
gained acceptability in the ICU based on a single,unblinded, non-randomized study in which IV adminis-tration produced fewer extrapyramidal side effects (com-pared with enteral haloperidol) in 10 patients [13].
Intravenous (IV) administration of haloperidol has
gained acceptability in the ICU based on a single,unblinded, non-randomized study in which IV adminis-tration produced fewer extrapyramidal side effects (com-pared with enteral haloperidol) in 10 patients [13].