Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Src patient history form
PINNACLE SPORTS PERFORMANCE AND REHABILITATION PATIENT HISTORY FORM Name: ____________________________ Date: ____________________________ DOB: _________________________ Chief Complaint:
Pain in: Head Neck Shoulder Arm Mid back
FOR PROVIDER USE ONLY
Low back Buttock Leg Other__________________
History of Present Illness: When did your pain begin?______________________ work-related?
No apparent reason Bending Lifting Fall
Have you had a similar episode before? Yes No
What have you been told is wrong? _____________________________
Prior tests for your pain: Test/Results:
X-ray______________________________________________________
MRI_______________________________________________________
CT________________________________________________________
Lab_______________________________________________________ Other______________________________________________________
Prior treatment for your current problem:
Anti-inflammatory: Ibuprofen Aleve
Steroids: Cortisone pills Cortisone injection
Injections: Epidural Facet Other
Spinal surgery: Year/Procedures/Results__________________________
Physical therapy: Year/Procedures/Results__________________________
Year/Procedures/Results__________________________ _____________________________________
Other Treatments: Year/Type/Results _____________________________
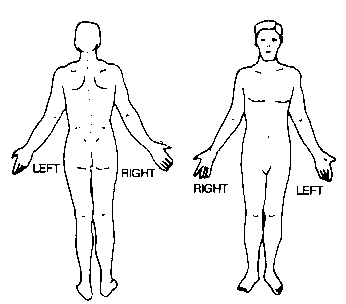
How do the following affect your pain? Please fill out the pain drawing below Use these symbols on the drawings: >>>> Ache
Numbness X X X X Burning 0 0 0 0 Pins and Needles ///////// Stabbing What level would you rate your pain right now? (please circle) None 0 1 2 3 4 5 6 7 8 9 10 Most severe Family Medical History: Heart disease Cancer Lupus Diabetes
Arthritis Abnormal bleeding Muscle disease Scoliosis
Rheumatoid Arthritis Drug allergies Other ________________________ ____
Living parents? Mother Yes No; Died at age ______ of _____________ _____________________________________
Father Yes No; Died at age ______ of _____________
Name: __________________________ Date: ______________________________ DOB: _______________________ Current Work Status: Employer ______________________________ Job Title________________________ Time at this position ______________________ Regular Duty Modified Duty - Date began:_____________________ Off work – Date began:____________________ Description of your Normal Job Activities
Standing
* If lifting at work, what is the average weight? ________________lbs. How many times per hour? __________________
Lifestyle Habits: FOR PROVIDER USE ONLY
How long have you smoked? ________________ (years)
Alcohol _____ (# of drinks/day) Caffeine beverages _______ (#/day) Are you currently exercising regularly? Yes; how long: ______________
No; last regular exercise:__________
Has your condition prevented you from doing exercise? Yes No
Past Medical History:
Cancer Arthritis Alcoholism Kidney disease
Glaucoma Heart Disease Tuberculosis
AIDS/HIV Hepatitis Diverticulitis High Blood Pressure
Surgeries/Hospitalizations: Injuries/Fractures/Dislocations: List all medications you are currently taking: __________________ Drug Allergies: No Yes; ____________________________________ Review of Systems: (Please check all that apply):
Ears, Mouth, and Throat: Abrupt change in hearing Difficulty swallowing
Urinary tract Respiratory Skin
Immune system dysfunction Other ____________
Depression Anxiety Difficulty sleeping
SAMPLE ITEMS BLOCK 1, ITEMS 1-50 A healthy 25-year-old man is undergoing an An otherwise healthy 3-week-old boy is brought exercise stress test. Which of the following is to the physician's office because of jaundice and most likely to occur in this man's skeletal muscle hepatomegaly, and his stools are loose, clay-colored, and acholic. Serum conjugated bilirubin (A) Decreased ca
Brief CV of M A Zanjanchi Biography: Date of birth: June 1954 Place of birth: Ghazvin, Iran Nationality: Iranian Marital status: Married, two daughters and one son Affiliation and working address: Department of Chemistry, Faculty of Science, University of Guilan, P.O. Box 1914, Rasht, Iran Tel: 0131-3243630-5 Fax: 0131-3220066 E-mail Academic Ranks: Assistant Prof. 1982-1996 A
 PINNACLE SPORTS PERFORMANCE AND REHABILITATION PATIENT HISTORY FORM
PINNACLE SPORTS PERFORMANCE AND REHABILITATION PATIENT HISTORY FORM