Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Medical complications of psychiatric illness/treatment
expectancy compared to the general population
• Majority of this is due to cardiovascular
• 80% of schizophrenics worldwide smoke • 30% of known diabetics, 62% of
hypertensives and 88% of hyperlipidemics were not receiving treatment at enrollment in CATIE trial.
• 20% SMI are infected with HCV • Between 1988 and 2002 rates of obesity
and diabetes in schizophrenics increased 6% to 19%
• Polypharmacy should be minimized • Generally no indication for >1 SSRI/SNRI,
>1 atypical antipsychotic, or >1 BZD
• In Bipolar illness often need medications
from multiple classes and can use multiple mood stabilizers.
– Addition of WBT to an SSRI – Addition of atypical antipsychotic to SSRI – Addition Thyroid hormone
– Addition low dose Lithium – Addition Folate – Addition SAMe – Addition Lamotrigine
• Mood Stabilizers • Antipsychotics • Antidepressants
• Typical (First Generation) Antipsychotics • Atypical (Second Generation)
• Mood Stabilizers • Antidepressants
(Zyprexa)> Quetiapine (Seroquel), Risperidone (Risperdal)>Aripiprazole (Abilify)> Ziprazidone (Geodon)
• Metabolic side effects- wt gain, diabetes,
hyperlipidemia listed above in decreasing order of risk for these complications
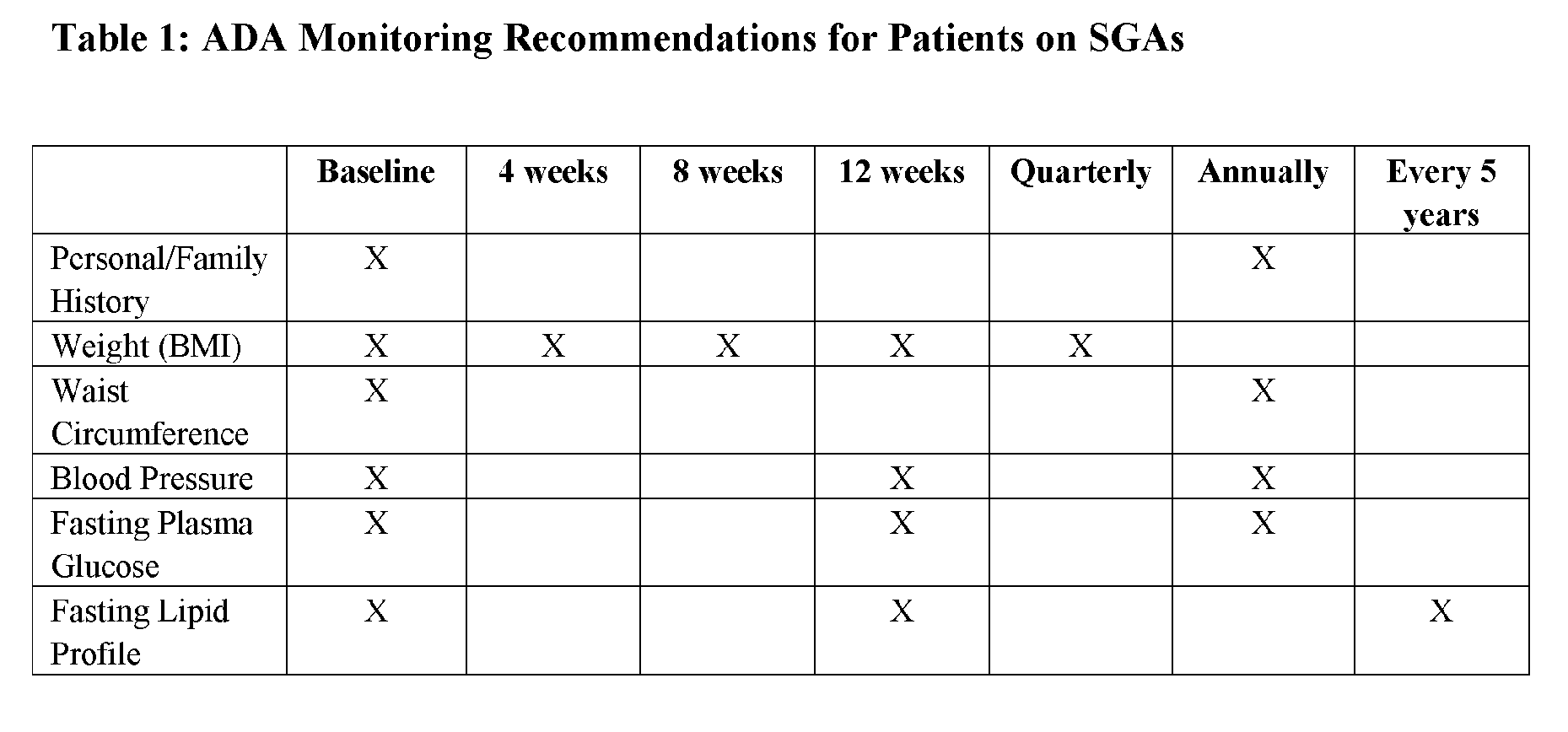
came up with consensus guidelines for atypical antipsychotic screening (see next slide).
– Diabetics started on atypical antipsychotics monitored
– If RF for DM get baseline and periodic fasting glucose
– Any pt placed on atypical antipsycotic monitored for
sx’s of hyperglycemia if sx’s get fasting glucose
• Haldol, Prolixin, etc (but remember atypicals
also can cause these SE’s at a lower rate)
– Dystonic rxn within hours (treat with IM/IV benadryl) – Akithesia within days to weeks (Treat with
– Parkinsonism within months to years (treat with
– fever, muscular rigidity, altered mental status, and
– 90% cases occur within 10 days of initiation of med
• QT prolongation • Hyperprolactenemia
– Gynecomastia, decreased libido, amenorrhea – Most commonly from Risperidone/Invega/typical
• Orthostatic Hypotension • Anticholinergic side effects
• Leukopenia/Agranulocytosis- weekly CBC
for 6 months then q2wk CBC for 6 months then monthly CBC.
• Drooling (Sialorrhea) • Siezures • Similar to Zyprexa in metabolic effects
• Probably most effective tx for classic Bipolar I • Renally cleared only • Narrow therapuetic window • Initial labs: BMP, TSH • BMP, TSH, Li level q6-12 months • Therapuetic serum level 0.6-1.2 (check 12h after
• Common maintinence doses 600-1500mg/day • QHS dosing optimal
– Tremor – Polyuria – GI (nausea/diarrhea)
• Toxicity- continued use of lithium with renal insufficiency
most common cause, lithium levels above 1.0 can cause toxicity
• Sxs of toxicity: ataxia, confusion, nausea/vomiting • Toxicity requires hospitalization for telemetry • Hypothyroidism
– Generally not severe, often will treat with synthroid and can keep
• Diabetes Insipidus • Hypercalcemia • Renal Failure?
– Many medications can increase Lithium
– Avoid NSAIDs, diuretics, ACE/ARB unless
you are carefully monitoring lithium level
– Anything that decreases renal fxn can cause
• Treatment for Bipolar d/o • Common maintenance doses 1000-2500mg/day • Serum levels used for dosing; therapuetic serum
level 60-125 (drawn 12h after last dose)
• Baseline labs: CBC, LFTs. • Monitor CBC, LFTs, Valproic acid level q6-12
• Ammonia level if symptomatic (note ammonia
level often elevated in asymptomatic patients on Depakote)
– Nausea/diarrhea – Wt gain – Sedation – Thrombocytopenia – Alopecia
– Would not rec in women of child bearing age – If you do us it in this population put in an IUD
• Pancreatitis • Polycystic ovary syndrome • Pancytopenia • Encephalopathy
– Many drug-drug interactions – Autoinducer therefore levels will decrease over time – Lab monitoring: tegretol level, CBC, LFTs, sodium – Side effects: hyponatremia, SJS, liver tox, pancytopenia,
– SJS, d/c med if develops rash, most common in asians
– Metabolic acidosis – Wt loss – “dopamax”
– Sexual side effects (anorgasmia, decreased libido) – Hyponatremia – Serotonin Syndrome (requires 3 of below)
• • Diarrhea • Heavy sweating not due to activity • Fever • Mental status changes such as or hypomania • Muscle spasms (myoclonus) • Overactive reflexes ( • Shivering • Tremor • Uncoordinated movements (ataxia)
– Initial anxiety (for first 2 weeks) – Mania/hypomania
– Wt gain – Discontinuation syndrome – FDA warning for birth defects
• Wt gain: Mirtazapine>paxil>zoloft, celexa,
• Sedation: Mirtazapine>paxil, zoloft>celexa,
• Drug/Drug interactions: Prozac, Paxil have the
most; Lexapro, Celexa, Zoloft have the least.
• Sexual side effects: Wellbutrin and Mirtazapine
only two antidepressants without sexual SE’s
• Elderly: celexa, lexapro, zoloft, remeron • Pregnant: zoloft (but probably would not change
any antidepressant if pt is responding to it except maybe paxil)
• Children/Adolescents: Prozac, Lexapro • Multiple medical problems: celexa, zoloft,
• Concurrent anxiety: SSRI • Concurrent ADHD: WBT • Chronic/Neuropathic Pain: Effexor, Cymbalta,
• Nortriptyline best choice in elderly due to
sedation, wt gain, constipation, urinary retention
• Not a good choice in those with cardiac dz • Good effectiveness for chronic pain
• Tranylcypromine (Parnate), Phenelzine (Nardil),
Isocarboxazid (Marplan), Selegiline (EMSAM)
• EMSAM transdermal patch 6mg and less no
• Otherwise all MAOIs require adherence to low
tyramine diet to avoid hypertensive crisis
• Never combine SSRI and MAOI • Always check for drug/drug interations when
prescribing a medication to a person on MAOI
– SSRI but rarely used except sometimes for
• Use great care when combining TCAs and
SSRIs the SSRI will increase the TCA level
• Tramadol and SSRI/WBT increase sz risk,
• Never combine MAOI and SSRI • Avoid TCAs in heart dz • Avoid combining triptans and SSRIs
FORMULAIRE D’AUTORISATION PRÉALABLE POUR REMBOURSEMENT SVP envoyer le formulaire Pour le traitement de la dysfonction érectile : Viagra (sildenafil), par télécopieur au : 1-866-840-1509 Cialis (tadalafil), Levitra (vardenafil) et Staxyn (vardenafil) Le patient ET le médecin doivent remplir le formulaire. Tous les champs du formulaire sont obligatoires et doivent être r
GERIATRIC GYNECOLOGY Karen L. Miller, MD; Morton A. Stenchever, MD; Holly E. Richter, PhD, MD; Evelyn C. Granieri, MD, MPH, MSEd; William C. Andrews, MD, FACOG, FRCOG* Gynecologists play three roles in the health care of women aged 65 and over: surgeon,consultant and therapist for gynecologic disorders, and provider of primary and preventivehealth care. The research reviewed here addresse
 • Haldol, Prolixin, etc (but remember atypicals
also can cause these SE’s at a lower rate)
– Dystonic rxn within hours (treat with IM/IV benadryl) – Akithesia within days to weeks (Treat with
– Parkinsonism within months to years (treat with
– fever, muscular rigidity, altered mental status, and
– 90% cases occur within 10 days of initiation of med
• QT prolongation • Hyperprolactenemia
– Gynecomastia, decreased libido, amenorrhea – Most commonly from Risperidone/Invega/typical
• Orthostatic Hypotension • Anticholinergic side effects
• Leukopenia/Agranulocytosis- weekly CBC
for 6 months then q2wk CBC for 6 months then monthly CBC.
• Drooling (Sialorrhea) • Siezures • Similar to Zyprexa in metabolic effects
• Probably most effective tx for classic Bipolar I • Renally cleared only • Narrow therapuetic window • Initial labs: BMP, TSH • BMP, TSH, Li level q6-12 months • Therapuetic serum level 0.6-1.2 (check 12h after
• Common maintinence doses 600-1500mg/day • QHS dosing optimal
– Tremor – Polyuria – GI (nausea/diarrhea)
• Toxicity- continued use of lithium with renal insufficiency
most common cause, lithium levels above 1.0 can cause toxicity
• Sxs of toxicity: ataxia, confusion, nausea/vomiting • Toxicity requires hospitalization for telemetry • Hypothyroidism
– Generally not severe, often will treat with synthroid and can keep
• Diabetes Insipidus • Hypercalcemia • Renal Failure?
– Many medications can increase Lithium
– Avoid NSAIDs, diuretics, ACE/ARB unless
you are carefully monitoring lithium level
– Anything that decreases renal fxn can cause
• Treatment for Bipolar d/o • Common maintenance doses 1000-2500mg/day • Serum levels used for dosing; therapuetic serum
level 60-125 (drawn 12h after last dose)
• Baseline labs: CBC, LFTs. • Monitor CBC, LFTs, Valproic acid level q6-12
• Ammonia level if symptomatic (note ammonia
level often elevated in asymptomatic patients on Depakote)
– Nausea/diarrhea – Wt gain – Sedation – Thrombocytopenia – Alopecia
– Would not rec in women of child bearing age – If you do us it in this population put in an IUD
• Pancreatitis • Polycystic ovary syndrome • Pancytopenia • Encephalopathy
– Many drug-drug interactions – Autoinducer therefore levels will decrease over time – Lab monitoring: tegretol level, CBC, LFTs, sodium – Side effects: hyponatremia, SJS, liver tox, pancytopenia,
– SJS, d/c med if develops rash, most common in asians
– Metabolic acidosis – Wt loss – “dopamax”
– Sexual side effects (anorgasmia, decreased libido) – Hyponatremia – Serotonin Syndrome (requires 3 of below)
• • Diarrhea • Heavy sweating not due to activity • Fever • Mental status changes such as or hypomania • Muscle spasms (myoclonus) • Overactive reflexes ( • Shivering • Tremor • Uncoordinated movements (ataxia)
– Initial anxiety (for first 2 weeks) – Mania/hypomania
– Wt gain – Discontinuation syndrome – FDA warning for birth defects
• Wt gain: Mirtazapine>paxil>zoloft, celexa,
• Sedation: Mirtazapine>paxil, zoloft>celexa,
• Drug/Drug interactions: Prozac, Paxil have the
most; Lexapro, Celexa, Zoloft have the least.
• Sexual side effects: Wellbutrin and Mirtazapine
only two antidepressants without sexual SE’s
• Elderly: celexa, lexapro, zoloft, remeron • Pregnant: zoloft (but probably would not change
any antidepressant if pt is responding to it except maybe paxil)
• Children/Adolescents: Prozac, Lexapro • Multiple medical problems: celexa, zoloft,
• Concurrent anxiety: SSRI • Concurrent ADHD: WBT • Chronic/Neuropathic Pain: Effexor, Cymbalta,
• Nortriptyline best choice in elderly due to
sedation, wt gain, constipation, urinary retention
• Not a good choice in those with cardiac dz • Good effectiveness for chronic pain
• Tranylcypromine (Parnate), Phenelzine (Nardil),
Isocarboxazid (Marplan), Selegiline (EMSAM)
• EMSAM transdermal patch 6mg and less no
• Otherwise all MAOIs require adherence to low
tyramine diet to avoid hypertensive crisis
• Never combine SSRI and MAOI • Always check for drug/drug interations when
prescribing a medication to a person on MAOI
– SSRI but rarely used except sometimes for
• Use great care when combining TCAs and
SSRIs the SSRI will increase the TCA level
• Tramadol and SSRI/WBT increase sz risk,
• Never combine MAOI and SSRI • Avoid TCAs in heart dz • Avoid combining triptans and SSRIs
• Haldol, Prolixin, etc (but remember atypicals
also can cause these SE’s at a lower rate)
– Dystonic rxn within hours (treat with IM/IV benadryl) – Akithesia within days to weeks (Treat with
– Parkinsonism within months to years (treat with
– fever, muscular rigidity, altered mental status, and
– 90% cases occur within 10 days of initiation of med
• QT prolongation • Hyperprolactenemia
– Gynecomastia, decreased libido, amenorrhea – Most commonly from Risperidone/Invega/typical
• Orthostatic Hypotension • Anticholinergic side effects
• Leukopenia/Agranulocytosis- weekly CBC
for 6 months then q2wk CBC for 6 months then monthly CBC.
• Drooling (Sialorrhea) • Siezures • Similar to Zyprexa in metabolic effects
• Probably most effective tx for classic Bipolar I • Renally cleared only • Narrow therapuetic window • Initial labs: BMP, TSH • BMP, TSH, Li level q6-12 months • Therapuetic serum level 0.6-1.2 (check 12h after
• Common maintinence doses 600-1500mg/day • QHS dosing optimal
– Tremor – Polyuria – GI (nausea/diarrhea)
• Toxicity- continued use of lithium with renal insufficiency
most common cause, lithium levels above 1.0 can cause toxicity
• Sxs of toxicity: ataxia, confusion, nausea/vomiting • Toxicity requires hospitalization for telemetry • Hypothyroidism
– Generally not severe, often will treat with synthroid and can keep
• Diabetes Insipidus • Hypercalcemia • Renal Failure?
– Many medications can increase Lithium
– Avoid NSAIDs, diuretics, ACE/ARB unless
you are carefully monitoring lithium level
– Anything that decreases renal fxn can cause
• Treatment for Bipolar d/o • Common maintenance doses 1000-2500mg/day • Serum levels used for dosing; therapuetic serum
level 60-125 (drawn 12h after last dose)
• Baseline labs: CBC, LFTs. • Monitor CBC, LFTs, Valproic acid level q6-12
• Ammonia level if symptomatic (note ammonia
level often elevated in asymptomatic patients on Depakote)
– Nausea/diarrhea – Wt gain – Sedation – Thrombocytopenia – Alopecia
– Would not rec in women of child bearing age – If you do us it in this population put in an IUD
• Pancreatitis • Polycystic ovary syndrome • Pancytopenia • Encephalopathy
– Many drug-drug interactions – Autoinducer therefore levels will decrease over time – Lab monitoring: tegretol level, CBC, LFTs, sodium – Side effects: hyponatremia, SJS, liver tox, pancytopenia,
– SJS, d/c med if develops rash, most common in asians
– Metabolic acidosis – Wt loss – “dopamax”
– Sexual side effects (anorgasmia, decreased libido) – Hyponatremia – Serotonin Syndrome (requires 3 of below)
• • Diarrhea • Heavy sweating not due to activity • Fever • Mental status changes such as or hypomania • Muscle spasms (myoclonus) • Overactive reflexes ( • Shivering • Tremor • Uncoordinated movements (ataxia)
– Initial anxiety (for first 2 weeks) – Mania/hypomania
– Wt gain – Discontinuation syndrome – FDA warning for birth defects
• Wt gain: Mirtazapine>paxil>zoloft, celexa,
• Sedation: Mirtazapine>paxil, zoloft>celexa,
• Drug/Drug interactions: Prozac, Paxil have the
most; Lexapro, Celexa, Zoloft have the least.
• Sexual side effects: Wellbutrin and Mirtazapine
only two antidepressants without sexual SE’s
• Elderly: celexa, lexapro, zoloft, remeron • Pregnant: zoloft (but probably would not change
any antidepressant if pt is responding to it except maybe paxil)
• Children/Adolescents: Prozac, Lexapro • Multiple medical problems: celexa, zoloft,
• Concurrent anxiety: SSRI • Concurrent ADHD: WBT • Chronic/Neuropathic Pain: Effexor, Cymbalta,
• Nortriptyline best choice in elderly due to
sedation, wt gain, constipation, urinary retention
• Not a good choice in those with cardiac dz • Good effectiveness for chronic pain
• Tranylcypromine (Parnate), Phenelzine (Nardil),
Isocarboxazid (Marplan), Selegiline (EMSAM)
• EMSAM transdermal patch 6mg and less no
• Otherwise all MAOIs require adherence to low
tyramine diet to avoid hypertensive crisis
• Never combine SSRI and MAOI • Always check for drug/drug interations when
prescribing a medication to a person on MAOI
– SSRI but rarely used except sometimes for
• Use great care when combining TCAs and
SSRIs the SSRI will increase the TCA level
• Tramadol and SSRI/WBT increase sz risk,
• Never combine MAOI and SSRI • Avoid TCAs in heart dz • Avoid combining triptans and SSRIs