Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Dialspace.dial.pipex.com
Journal of Clinical Endocrinology and Metabolism
Copyright 1998 by The Endocrine Society
The Dexamethasone-Suppressed Corticotropin-Releasing Hormone Stimulation Test Differentiates Mild Cushing’s Disease from Normal Physiology
JACK A. YANOVSKI*†, GORDON B. CUTLER, JR.†, GEORGE P. CHROUSOS, ANDLYNNETTE K. NIEMAN
Office of the Director (J.A.Y.), Warren Grant Magnuson Clinical Center and The DevelopmentalEndocrinology Branch (J.A.Y., G.B.C, G.P.C., L.K.N.), National Institute of Child Health and HumanDevelopment, National Institutes of Health, Bethesda, Maryland 20892-1862ABSTRACT
0.001) but within the normal range (55–250 nmol/day) in 4 patients.
The dexamethasone-suppressed CRH test (Dex-CRH test) differ-
During low-dose dexamethasone suppression, a UFC less than 100
entiates patients with Cushing’s syndrome (CS) from those with pseu-
nmol/day (36 g/day) was found in all but 1 volunteer subject, and a
do-Cushing states, who have decreased ACTH responses to CRH
urine 17-hydroxycorticosteroid excretion less than 14.6 mol/day (5.3
because of negative feedback exerted by chronic hypercortisolism.
mg/day) was found in all but 2 subjects. During the Dex-CRH test,
Normal subjects, however, have not been studied with the Dex-CRH
plasma cortisol less than 38 nmol/L was found in all 20 normal vol-
test, raising concern that this test might not separate patients with
unteers until 30 min after CRH administration. By contrast, the
CS from patients with normal adrenal function. To determine
15-min CRH-stimulated plasma cortisol exceeded 38 nmol/L in all
whether the criterion that separates CS from pseudo-Cushing states
patients with CD (P Ͻ 0.001). Plasma dexamethasone measured just
also would differentiate patients with Cushing’s disease (CD) from
before CRH administration was similar in normal volunteers (13.0 Ϯ
individuals with eucortisolism, we studied 20 healthy volunteers dur-
6.1 mol/L) and patients with CD (16.4 Ϯ 6.4 mol/L). We conclude
ing low-dose (2 mg/day) dexamethasone suppression, and then during
that cortisol measurements obtained during the Dex-CRH test are
the Dex-CRH test (CRH stimulation test performed 2 h after com-
suppressed in normal volunteers below those found in mild CD. These
pletion of low-dose dexamethasone suppression), and contrasted their
results suggest that the Dex-CRH test may be useful in the evaluation
results with those of 20 patients with surgically proven mild CD
of CS in patients without significant hypercortisoluria. However, its
[urine free cortisol (UFC) Ͻ1000 nmol/day).
value in patients with episodic hormonogenesis has not been tested.
Basal UFC was significantly greater in patients with CD (P Ͻ
(J Clin Endocrinol Metab 83: 348 –352, 1998)
SEVERALtestsarecurrentlyinclinicalusetodifferen- sone-suppressed CRH (Dex-CRH) test. In a pilot study, 39
tiate Cushing’s syndrome (CS) from conditions caus-
patients with CS and 19 patients believed to have PCS were
ing pseudo-Cushing states (PCS), such as depression,
given dexamethasone (0.5 mg/dose every 6 h for 8 doses)
stress, renal failure, alcoholism, or obesity. The low-dose
followed by administration of 1 g/kg ovine CRH 2 h after
dexamethasone suppression test (1–3) measures 17-
the last dose of dexamethasone. In this study, a plasma cor-
hydroxycorticosteroid excretion during administration of
tisol value (measured 15 min after CRH administration) that
dexamethasone, 0.5 mg every 6 h for 2 days. When 17-
was greater than 38 nmol/L had 100% diagnostic accuracy
hydroxycorticosteroid excretion exceeds 11.0 mol/day (4
for CS, and the Dex-CRH test had superior sensitivity and
mg/day) (4), the test is considered positive for CS. How-
diagnostic accuracy when compared either with the low-
ever, this test may misclassify as many as 15% of patients
dose dexamethasone suppression test or with the CRH test
with CS and up to 15% of patients with PCS (5). The CRH
stimulation test, valuable in differentiating the syndrome
Patients with PCS have decreased ability to secrete
of ectopic ACTH from Cushing’s disease (CD) (6, 17), is
ACTH in response to CRH because of the glucocorticoid
also of limited use in the differential diagnosis between
negative feedback exerted by chronic hypercortisolism
PCS and CD because there is considerable overlap with the
(11). However, many patients referred for endocrinologic
responses of patients with CD (5, 7–9). Other tests to dis-
evaluation, to rule out CS, either have no evidence for
tinguish CD from PCS have been described but not fully
hypercortisoluria, or minimal elevation of urine free cor-
tisol (UFC) or 17-hydroxycorticosteroids (17OHCS). Be-
The lack of a test with both high sensitivity and high
cause such individuals have not been exposed to chronic
specificity for CS led to the development of the dexametha-
hypercortisolism, they might have a greater ACTH andcortisol response to the Dex-CRH test than those with a
Received March 17, 1997. Revision received May 15, 1997. Rerevision
sustained PCS. To determine whether the criterion that
received July 22, 1997. Accepted October 24, 1997.
separates CS from PCSs also will distinguish CS from
* To whom correspondence and requests for reprints should be ad-
individuals without hypercortisolism, we compared the
dressed, at Building 10, Room 10N262, National Institutes of Health,
results of the Dex-CRH test in 20 normal volunteers and
Bethesda, Maryland 20892-1862. E-mail: [email protected].
† Commissioned officers in the U.S. Public Health Service. Subjects and Methods
Data were analyzed on a Macintosh Power PC using SuperAnova and
Twenty volunteers (22–58 yr old; 10 males and 10 females) were
StatView 4.5 (Abacus Concepts, Inc., Berkeley, CA), and RuleMaker
recruited through posted notices in the Bethesda, MD area (Table 1).
(Digital, Hanover, MA). After logarithmic data transformation, ANOVA
Twenty patients with surgically-proven CD were referred to NIH for
(with repeated measures) was performed for plasma cortisol and plasma
evaluation of mild hypercortisolism (UFC Ͻ 1000 nmol/day; normal
ACTH measurements, employing a conservative (Greenhouse-Geisser)
range: 50 –250 nmol/day) between May 1992 and February 1994, and
F test. The relation between the dexamethasone level and plasma cortisol
have not been the subjects of any prior report. These 20 patients un-
was determined by simple regression. After dexamethasone adminis-
derwent biochemical tests to determine the cause of their CS (12, 13, 14,
tration, UFC and 17OHCS were not normally distributed, and they were
15). Based on results of testing, they underwent transsphenoidal pitu-
analyzed using the Mann-Whitney nonparametric test using the Bon-
itary exploration, which revealed an adenoma with ACTH staining in
ferroni correction for multiple comparisons. Tabular data are presented
each case. All normal volunteers were medication-free for at least 2
weeks before the start of the study, and all were free of significant
Estimates of sensitivity, specificity, positive predictive value, nega-
medical disease. None of the normal volunteers had evidence of any
tive predictive value, and diagnostic accuracy were determined for each
psychiatric disorder known to affect the hypothalamic-pituitary adrenal
test statistic (16). The sensitivity and diagnostic accuracy of each of the
axis, and all had refrained from the use of any steroid preparation for
test criteria were compared at 100% specificity by -square statistics (17).
a minimum of 3 months before study. The study was approved by the
We compared the criteria for the diagnosis of CD of the various tests,
NIH Intramural Clinical Research Subpanel, and each subject gave writ-
using cut-points with 100% specificity for the diagnosis of CS from PCS
found in our previous retrospective study (5).
In all subjects, the 24-h excretion of UFC, 17OHCS, and creatinine was
Low-dose dexamethasone suppression
measured for 1 day while subjects took no glucocorticoids, and subse-
Urine 17-hydroxycorticosteroid and free cortisol were
quently, during administration of 0.5 mg dexamethasone orally every 6 h
measured before and during dexamethasone administration
A Dex-CRH test was performed in all subjects, starting 2 h after the
in all subjects. Both urine 17-hydroxycorticosteroid and free
patient had completed dexamethasone treatment. Ovine CRH (Bachem,
cortisol excretion were significantly greater in patients with
Torrence, CA) was administered as an iv bolus injection at a dose of 1
CD (Table 1, P Ͻ 0.001). UFC was within the normal range
g/kg between 0800 and 0810 h. Plasma samples were assayed for
(55–250 nmol/day) in 4 of the 20 patients with CD (none with
cortisol and ACTH at Ϫ15, Ϫ10, Ϫ5, and Ϫ1 min before CRH stimulationand then at 5, 15, 30, 45, and 60 min after CRH; and for dexamethasone,
episodic hypersecretion of cortisol), and greater than the
at Ϫ1 min. Normal volunteers underwent CRH testing in the endocrine
normal range in 1 normal volunteer (290 nmol/L).
outpatient clinic. Patients with CD were admitted to the inpatient en-
Both UFC and 17OHCS decreased significantly after dexa-
docrinology ward of the Warren Grant Magnuson NIH Clinical Center
methasone administration in both groups (Tables 2 and 3,
P Ͻ 0.001). During the second day of dexamethasone sup-
pression, one normal volunteer had a UFC greater than 100nmol/day (36 g/day), and two normal volunteers had
UFC, 17OHCS, and creatinine were measured as previously described
urine 17-hydroxycorticosteroid excretion more than 14.6
(12). The intraassay and interassay variabilities were 8–12% and 8–15% for
mol/day (5.3 mg/day). These values represented cut-
UFC, 6–12% and 7–20% for 17OHCS, and 1% and 2% for creatinine. Dailycreatinine measurements varied by no more than 10%. Plasma ACTH and
points with 100% specificity for the diagnosis of CS in our
cortisol were measured, as previously described (6), by Corning Hazleton
previous retrospective study (5). Use of lower values of uri-
Laboratories (Vienna, VA). The sensitivity for the ACTH assay ranged from
nary 17OHCS or UFC as the cut-points for the diagnosis of
0.9–2.2 pmol/L and for cortisol, from 5.5–22 nmol/L. The intraassay and
CD yielded similar results: a 17-hydroxycorticosteroid more
interassay variabilities were 7–12% and 12–25% for ACTH, and 6 and 15%for cortisol. Each cortisol sample also was measured in a second, serum
than 6.9 mol/day (2.5 mg/day) for the diagnosis of CD had
cortisol assay, performed by the Clinical Pathology Laboratory of the NIH
90% sensitivity and 65% specificity; a UFC criterion more
Clinical Center, using the Abbott TDX kit (Abbot Park, IL). Results were
than 56 nmol/day (20 g/day) had 75% sensitivity and 93%
equivalent, except that Abbott kit cortisol determinations had a higher limit
specificity for the diagnosis of CD.
of detection (27.6 nmol/L) than those measured at Corning Hazleton Lab-oratories (5.5–22 nmol/L). In this report, results from the Corning HazletonLaboratories plasma cortisol assay are given. Plasma samples were assayed
CRH test with dexamethasone pretreatment (Dex-CRH test)
for dexamethasone by Endocrine Sciences (Calabasas Hills, CA). The in-traassay and interassay variabilities for the plasma dexamethasone assay
All subjects completed the Dex-CRH test (Fig. 1, Tables 2
and 3). ANOVA showed significant group-by-time interac-
TABLE 1. Study patients
18 Caucasian, 1 Hispanic, 1 Pacific Islander
Basal 24-h urine-free cortisol excretion, nmol/day
Basal 17-hydroxycorticosteroid excretion, mol/day
a P Ͻ 0.001 Cushing disease vs. healthy volunteers. TABLE 2. Results following dexamethasone suppression
Dexamethasone-suppressed urine-free cortisol excretion, nmol/day
Dexamethasone-suppressed17-hydroxycorticosteroid excretion, mol/day
Dexamethasone-suppressed basal plasma cortisol, nmol/L
Dexamethasone-suppressed plasma cortisol 15 min after CRH, nmol/L
a P Ͻ 0.001 vs. measurement before administration of dexamethasone. b P Ͻ 0.001 Cushing disease vs. healthy volunteers.
min after CRH stimulation (Fig. 2B). The criterion for dex-amethasone-suppressed plasma ACTH that was best for dis-tinguishing CD was a plasma ACTH more than 3.5 pmol/Lat 30 min (Fig. 2C), which had 100% specificity and 90%sensitivity for the diagnosis of CD. Results using peak ACTHor peak cortisol response did not have 100% diagnosticaccuracy.
The mean plasma dexamethasone level (Table 2) measured
just before CRH administration did not differ for normalvolunteers (13.0 Ϯ 6.1 mol/L; 469.5 Ϯ 220.4 ng/dL) andpatients with CD (16.4 Ϯ 6.4 mol/L; 614.8 Ϯ 233.1 ng/dL). The two normal volunteers, whose plasma cortisol exceeded38 nmol/L at 45 and 60 min after CRH, had the two lowestplasma dexamethasone values (6.90 and 4.03 mol/L). Inpatients with CD, dexamethasone levels and plasma ACTHor cortisol measurements were not correlated, either at basalor CRH-stimulated time points (P ϭ 0.41, data not shown).
When compared, at criteria yielding 100% specificity for
FIG. 1. Results of CRH stimulation testing with low-dose dexameth-
the diagnosis of CD, the Dex-CRH test 15-min cortisol con-
asone pretreatment. Plasma ACTH in patients with CD (A) and in
centration had significantly greater sensitivity and diagnos-
normal volunteers (C). Plasma cortisol in patients with CD (B) and in
tic accuracy than dexamethasone-suppressed urine 17-hy-
normal volunteers (D). Means and SE of measurement are shown
droxycorticosteroid or free cortisol measurements (Table 3).
when SEM is greater than size of data point. F, CD; E, healthy vol-unteers; *, P
Although basal plasma cortisol after dexamethasone admin-
Ͻ 0.001, CD vs. healthy volunteers. Note differing y-axis
scaling for CD and for normal volunteers, which is required to show
istration did not correctly identify four patients with CD, this
80% sensitivity, when compared with the 100% sensitivity ofthe CRH-stimulated plasma cortisol level, was not statisti-
tions (P Ͻ 0.001). Plasma ACTH increased significantly in
cally significant (P ϭ 0.3). Similar results were found using
both groups (basal ACTH: 6.47 Ϯ 3.0, peak ACTH: 25.2 Ϯ 27.1
peak CRH-stimulated ACTH, ACTH 30 min after CRH stim-
pmol/L, P Ͻ 0.001 for CD; basal ACTH: 1.19 Ϯ 0.05, peak
ulation, or peak CRH-stimulated cortisol values (Table 3).
ACTH: 1.56 Ϯ 0.14 pmol/L, P Ͻ 0.04 for normal volunteers). Plasma cortisol rose significantly in patients with CD (basal
Discussion
cortisol: 156.14 Ϯ 41.64, peak cortisol: 471.58 Ϯ 67.02 nmol/L,
In this study, the Dex-CRH test (a new test for the differ-
P Ͻ 0.001) but did not change significantly in normal vol-
ential diagnosis of hypercortisolism) distinguished all pa-
unteers (basal cortisol: 27.29 Ϯ 0.83, peak cortisol: 31.92 Ϯ
tients with mild CD from healthy volunteers, using criteria
2.57 nmol/L, P ϭ 0.07). Both plasma ACTH and cortisol were
previously established to discriminate pseudo-Cushing
significantly greater in patients with CD at all time points
states from CD. The Dex-CRH-stimulated cortisol value, ob-
tained 15 min after administration of CRH, had better diag-
As was previously observed in individuals with PCS, a
nostic accuracy for the diagnosis of CD than either basal 24-h
Dex-CRH test plasma cortisol concentration less than 38
urine 17-hydroxycorticosteroid measurements or dexameth-
nmol/L was found in all 20 normal volunteers, both basally
asone-suppressed urine measurements. Although the 15-min
and at all times between 0 and 30 min after administration
Dex-CRH test did not have significantly greater diagnostic
of CRH (Fig. 1). The plasma cortisol of 2 normal volunteers
accuracy than basal UFC (P ϭ 0.06), basal dexamethasone-
exceeded 38 nmol/L at 45 and 60 min after CRH. A plasma
suppressed plasma cortisol (P ϭ 0.3), peak dexamethasone-
cortisol less than 38 nmol/L was found before administration
suppressed plasma cortisol (P ϭ 0.6), or Dex-CRH plasma
of CRH in 4 patients with CD (Fig. 2A); but in all cases, a
ACTH (P ϭ 0.6), the Dex-CRH test 15-min cortisol criterion
cortisol concentration in excess of 38 nmol/L was found 15
was the only evaluated criterion with both 100% specificity
TABLE 3. Comparison of tests
Comparison of criteria with 100% specificity for the diagnosis of Cushing disease. UFC, Urine free cortisol excretion; 17-OHCS, urine
a P Ͻ 0.05, vs. Dex-CRH test 15-min cortisol.
and sensitivity. Though the overnight 1-mg dexamethasonesuppression test would likely eliminate at least 90% of nor-mocortisoluric individuals from consideration of the diag-nosis of CS, the overnight 1-mg dexamethasone suppressiontest is of lesser value in differentiating individuals with PCSand CS (4). Because we wished to evaluate a test that coulddifferentiate patients with CS from all individuals withoutthe disorder, we did not perform the 1-mg test in the subjectsof the present study.
Most patients with CD show some suppression of ACTH
and cortisol by dexamethasone (6, 8, 12, 13, 18) and somestimulation of ACTH and cortisol by CRH (6, 14). However,cortisol secretion decreases greatly in some patients with CDduring low-dose dexamethasone, possibly because of slowdexamethasone clearance (19, 20). Such patients may be mis-classified as having PCS if evaluated only by suppression ofcortisol production after low-dose dexamethasone adminis-tration. In the present study, four subjects with CD haddexamethasone-suppressed basal plasma cortisol values lessthan 38 nmol/L. By the addition of CRH, to stimulate greaterACTH and cortisol secretion in patients with CD who areCRH-sensitive, those patients with unusual sensitivity todexamethasone suppression achieve greater ACTH and cor-tisol levels, above those of patients with PCS (5) or normalvolunteers. In this manner, the Dex-CRH test correctly iden-tifies more patients with CD than does low-dose dexameth-asone suppression, and therefore allows the criterion for thediagnosis of CS to be 100% specific, with a much highersensitivity than is possible with dexamethasone suppressionalone.
Four of the patients with CD in this study had basal UFC
excretion that was within the normal range. All four of thesepatients had Dex-CRH-stimulated cortisol levels greater thanthe 38 nmol/L cut-point identified in our previous study (5)and were correctly identified by the Dex-CRH test. In con-trast, healthy volunteers showed suppression of plasmaACTH and cortisol similar to that observed previously forpatients with PCS (5). These results lead us to believe that theDex-CRH test may be of value for determining who has trueCS among patients with normal, or only mildly elevated,UFC measurements. However, the value of the Dex-CRH test
FIG. 2. Individual data showing the criteria with the best diagnosticaccuracy. A, Basal plasma cortisol after dexamethasone-suppression;
in classifying those who have CS with periodic hormono-
B, Dex-CRH plasma cortisol obtained 15 min after CRH stimulation;
genesis (21–25), but who are not hypercortisolemic at the
C, Dex-CRH plasma ACTH obtained 30 min after CRH stimulation;
The observation that the lowest plasma dexamethasone
9. Rupprecht R, Lesch K, Muller U, et al. 1989 Blunted adrenocorticotropin but
levels in the study were found in the two normal volunteers,
normal -endorphin release after human corticotropin-releasing hormone ad-ministration in depression. J Clin Endocrinol Metab. 69:600 – 603.
whose Dex-CRH-stimulated plasma cortisol increased above
10. Bernini GP, Argenio GF, Cerri F, Franchi F. 1994 Comparison between the
38 nmol/L at 45 min, suggests that dexamethasone levels
suppressive effects of dexamethasone and loperamide on cortisol and
may aid interpretation of the Dex-CRH test. As with other
ACTH secretion in some pathological conditions. J Endocrinol Invest. 17:799 – 804.
tests that use dexamethasone, the Dex-CRH test should be
11. Yanovski JA. 1995 The dexamethasone-suppressed CRH test in the differential
interpreted with caution in patients receiving medications
diagnosis of Cushing disease and pseudo-Cushing states. The Endocrinologist.
that affect dexamethasone metabolism.
We conclude that plasma cortisol measurements obtained
12. Avgerinos PC, Yanovski JA, Oldfield EH, Nieman LK, Cutler Jr G. 1994 The
metyrapone and dexamethasone suppression tests for the differential diag-
during the Dex-CRH test are suppressed in normal volun-
nosis of the adrenocorticotropin-dependent Cushing syndrome: a comparison.
teers below those found in CD. Although its value in patients
with episodic hormonogenesis has not been demonstrated,
13. Flack MR, Oldfield EH, Cutler Jr GB, et al. 1992 Urine free cortisol in the
high-dose dexamethasone suppression test for the differential diagnosis of the
the Dex-CRH test may be useful in evaluating patients with
Cushing syndrome. Ann Intern Med. 116:211–217.
features of CS and little, or no, hypercortisoluria.
14. Nieman LK, Oldfield EH, Wesley R, Chrousos GP, Loriaux DL, Cutler Jr G.
1993 A simplified morning ovine corticotropin-releasing hormone stimulationtest for the differential diagnosis of adrenocorticotropin-dependent Cushing’s
Acknowledgments
syndrome. J Clin Endocrinol Metab. 77:1308 –1312.
15. Findling JW, Doppman JL. Biochemical and radiologic diagnosis of Cushing
We thank the nurses of the 10-West Endocrinology inpatient ward
syndrome. Endocrinol Metab Clin North Am. 23:511–537.
and the 9th floor outpatient clinic at the National Institutes of Health,
16. Swets JA. 1988 Measuring the accuracy of diagnostic systems. Science.
Barbara Filmore, and Shawnia Forrester for helping to carry out this
17. Beck JR, Shultz EK. 1986 The use of relative operating characteristic (ROC)
curves in test performance evaluation. Arch Pathol Lab Med. 110:13–20.
18. Dichek HL, Nieman LK, Oldfield EH, Pass HI, Malley JD, Cutler Jr G. 1994 References
A comparison of the standard high dose dexamethasone suppression test andthe overnight 8-mg dexamethasone suppression test for the differential diag-
1. Liddle G. 1960 Tests of pituitary-adrenal suppressibility in the diagnosis of
nosis of adrenocorticotropin-dependent Cushing’s syndrome. J Clin Endocri-
Cushing’s syndrome. J Clin Endocrinol Metab. 20:1539 –1561.
2. Eddy R, Jones A, Gilliland PF, et al. 1973 Cushing’s syndrome: a prospective
19. Caro JF, Meikle AW, Check JH, Cohen SN. 1978 “Normal Suppression” to
study of diagnostic methods. Am J Med. 55:621– 630.
dexamethasone in Cushing’s disease: an expression of decreased metabolic
3. Schteingart D. 1989 Cushing’s syndrome. Endocrinol Metab Clin North Am.
clearance for dexamethasone. J Clin Endocrinol Metab. 47:667– 670.
20. Kapcala LP, Hamilton SM, Meikle AW. 1984 Cushing’s disease with ’normal
4. Crapo LM. 1979 Cushing’s syndrome: a review of diagnostic tests. Metabolism.
suppression’ due to decreased dexamethasone clearance. Arch Intern Med.
5. Yanovski JA, Cutler Jr GB, Chrousos GP, Nieman LK. 1993 Corticotropin-
21. Brown RD, Van Loon GR, Orth DN, Liddle GW. 1973 Cushing’s disease with
releasing hormone stimulation following low-dose dexamethasone adminis-
periodic hormonogenesis: one explanation for paradoxical response to dexa-
tration: a new test to distinguish Cushing’s syndrome from pseudo-Cushing’s
methasone. J Clin Endocrinol Metab. 36:445– 451.
states. J Am Med Assoc. 269:2232–2238.
22. Yasuda K. 1996 Cyclic Cushing’s disease: pitfalls in the diagnosis and problems Nieman LK, Chrousos GP, Oldfield EH, Avgerinos PC, Cutler Jr G, Loriaux DL. 1986 The ovine corticotropin-releasing hormone stimulation test and the
with the pathogenesis. Intern Med. 35:169 –170.
dexamethasone suppression test in the differential diagnosis of Cushing’s
23. Hermus AR, Pieters GF, Borm GF, et al. 1993 Unpredictable hypersecretion
syndrome. Ann Intern Med. 105:862– 867.
of cortisol in Cushing’s disease: detection by daily salivary cortisol measure-
7. Gold PW, Loriaux DL, Roy A, et al. 1986 Physiology of hypercortisolism in
ments. Acta Endocrinol (Copenh). 128:428 – 432.
depression and Cushing’s disease. N Engl J Med. 314:1329 –1335.
24. Stewart PM, Venn P, Heath DA, Holder G. 1992 Cyclical Cushing’s syndrome.
8. Grossman A, Howlett T, Perry L, et al. 1988 CRF in the differential diagnosis
of Cushing’s syndrome: a comparison with the dexamethasone suppression
25. Shapiro MS, Shenkman L. 1991 Variable hormonogenesis in Cushing’s syn-
test. Clin Endocrinol (Oxf). 29:167–178.
ACTIONS EDUCATIVES ET VIE SCOLAIRE A.T.S.E.M. AGENTS SPECIALISES DES ECOLES MATERNELLES PUBLIQUES DE LA VILLE DE ROUEN JUIN 1998 - ASSISTANCE EDUCATIVE AU PERSONNEL ENSEIGNANT. - MISE EN ETAT DE PROPRETE DES MATERIELS ET DES LOCAUX OBJECTIF DE LA CHARTE La prÈsente charte est Ètablie en vue de dÈfinir les missions et de fixer les conditions de travaildes personnels des Èc
 TABLE 2. Results following dexamethasone suppression
TABLE 2. Results following dexamethasone suppression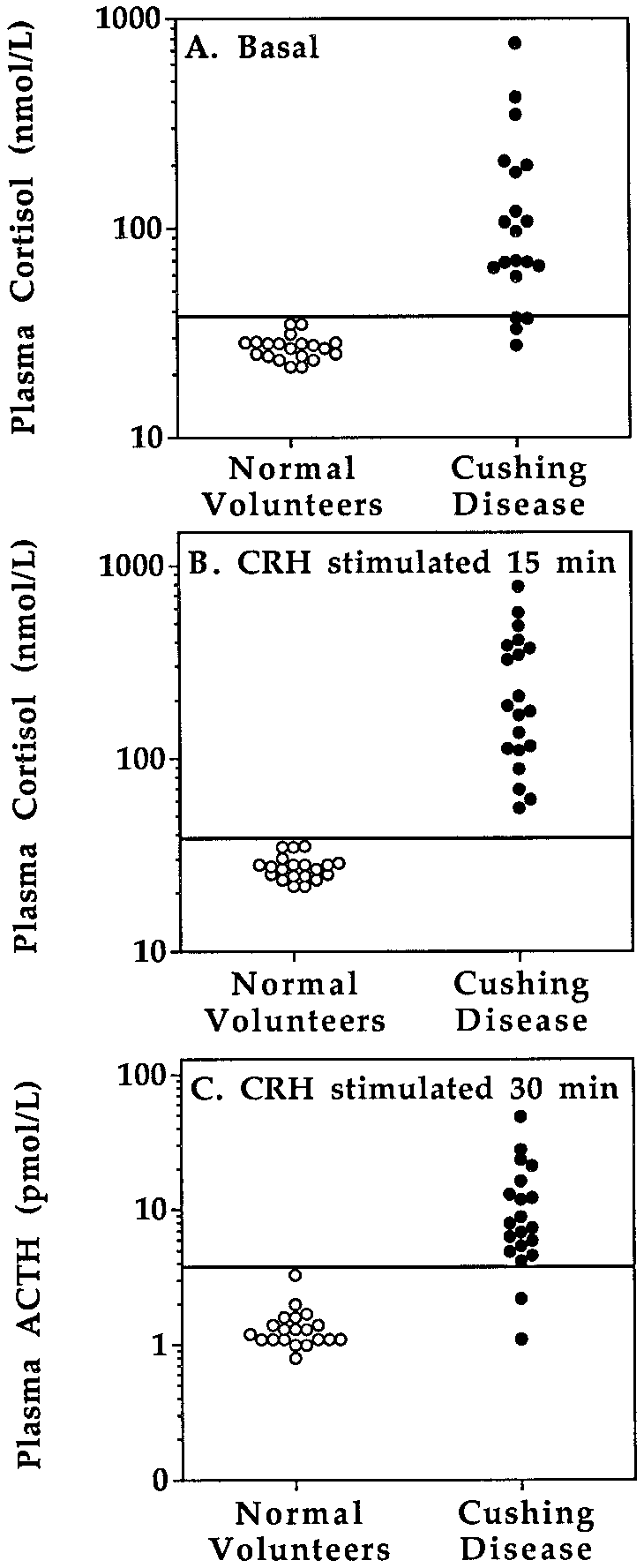 TABLE 3. Comparison of tests
TABLE 3. Comparison of tests