Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Radiology rounds june 2003 - ct colonography – an alternative to colonoscopy?
Radiology Rounds A Newsletter for Referring Physicians Massachusetts General Hospital Department of Radiology
CT Colonography – An Alternative to Colonoscopy?
Colorectal cancer is the third leading cause of cancer deaths in both men and women and the likelihood of
an individual developing it some point in his or her life
is about 6%. However, early stage colorectal cancer
can be successfully treated and the mortality benefit
of screening for colorectal cancer is well established.
Despite this, fewer than 40% of those for whom
screening is recommended comply and only about
37% of colorectal cancers are detected while the
Will CT colonography (CTC) be a way to improve the
screening rate and reduce the mortality from this
disease? A recent large prospective study has
demonstrated that it is at least as effective as the
current gold standard, optical colonoscopy, for
detecting adenomatous polyps (Pickhardt, Choi et al.
2003). At this time, both procedures require
preparatory bowel cleansing. However, colonography
is a better tolerated procedure that does not require
conscious sedation, which is necessary during the
optical colonoscopy examination. For this reason
alone, the availability of CT colonography may
Coronal reconstruction CT colonography image
improve compliance. In addition, in the cases in which
The air filled colon appears dark. Arrow indicates 1.5 cm
colonoscopy cannot, be completed due to stricture,
adenoma. Other soft tissue projections into the lumen of
obstruction, or the complex tortuosity of the colon, CT
the colon are normal haustral folds.
colonography has been established as the imaging
the "advanced adenomas" that represent the primary
Perhaps the most important disadvantage of CT
target of screening. The currently practiced, though
colonography is that any significant findings have to
more conservative approach is that lesions somewhat
be followed up by optical colonoscopy for polyp
less than 10 mm should also be resected, adding
removal. Hence, one may ask what the value of the
approximately another 10% of screening individuals
CTC is when any positive lesion detected by the new
who may be referred to colonoscopy. The value of
exam will require further referral? It is estimated that
colonography is in permitting the large fraction of the
six to nine percent of non-symptomatic patients over
at-risk screening populace who do not have significant
50 years may be expected to have a polyp greater
lesions to avoid the additional risk, discomfort, and
than 10 mm in size; lesions of this size range include
expense associated with conventional colonoscopy.
In studies that included more than 100 patients,
In comparison, studies of back-to-back colonoscopies
comparing the detection rate colonography with that of
performed on individual patients have demonstrated
colonoscopy, the reported per patient performance for
miss rates of about 6% for adenomatous polyps equal
detection of polyps equal to or greater than 10 mm
to or greater than 10 mm (the size above which lesions
ranged from 93-100% sensitivity and 80-100%
are considered to have a significant risk of harboring
specificity. The sensitivity per polyp in these studies
malignancy) and 13% for polyps in the 0.6-0.9 mm
ranged from 62-90% for polyps equal to or greater
range. These miss rates are comparable to results
than 10 mm and 16-82% for 6-9 mm polyps. False
achieved with state of the art CT colonography, as
positive results may occur because of retained stool,
diverticular disease, misinterpretation of thick or
complex haustral folds, and artifacts due to motion or
metal (e.g. hip prostheses). Colonography does,
however, have the potential advantage of identifying
cancers that may not be adequately assessed by
endoscopy, such as those that are located close to
Colonoscopy CT Colonography Patient preparation Patient tolerance Radiation Complications Visualization
Optical. Lesions identified by both color Tomographic and 3D reconstruction with
Localization Lesion removal *Current research is evaluating a procedure that does not require bowel cleansing. Instead, the patient must ingest a contrast agent with meals and snacks for two days. Computer image processing subtracts bowel contents for radiologist to view apparent empty bowel. This technique is currently in clinical trial.
The present CT colonographic procedure requires
Please note that CT colonography for cancer screening
purgative bowel cleansing with phospho-soda and
is not covered by most insurance at this time. CT
Bisacodyl (Fleet Prep Kit 1) or polyethylene glycol
colonography of asymptomatic patients can be
electrolyte solution (NuLytely® or Go-Lytely®). Prior
performed at MassGeneral West in Waltham or at
to the CT scan, an enema tip or catheter is placed in
the rectum and the colon filled with air until the
patient reports a full feeling. Few patients report any
( Internal Access Only )
more than minimal discomfort. Both supine and prone
CT images are acquired, which means that parts of
the colon that are compressed in one position are
open in the other. Current multi detector CT scanners
Instructions for patients on using the PEG
can acquire all the image data in two breath holds,
The whole procedure is complete within 15-20
minutes and, since there is no sedation, the patient is
able to resume normal activities immediately, before
the images are reviewed. The radiologist examines
If you have any patients who are interested in being
planar images of the entire length of the colon and
part of the clinical study of the minimally prepped CTC,
computer reconstruction of 3D images are made to
which requires both CTC with ingested contrast agent
view any part of the bowel from an angle that the
radiologist selects. The radiology report is sent to the
referring physician the same day of the procedure. 3D reconstruction image of normal colon.
Follow Up and TherapyUnlike colonoscopy, CT colonography is not
therapeutic. Therefore, all positive colonography scans
must be followed up by optical colonoscopy for polyp
removal or by surgery to remove larger masses. It
should be noted that the large majority of individuals
presenting for colon screening exam do not have
3D reconstruction image of colon.
significant polyps; CT colonography may permit these
individuals to avoid endoscopy while correctly and
more easily identifying those that require endoscopic
or surgical resection. If open surgery is necessary,
For further information about CT colonography, please
colonography has the advantage of indicating the
position of the lesion within the abdomen, making
ReferencesFidler, JL, Johnson, CD, MacCarty, RL, Welch, TJ,
Levin, B, Brooks, D, Smith, RA and Stone, A (2003).
Hara, AK and Harmsen, WS (2002). Detection of flat
Emerging technologies in screening for colorectal
lesions in the colon with CT colonography. Abdom
cancer: CT colonography, immunochemical fecal occult
Imaging 27: 292-300.
blood tests, and stool screening using molecular
markers. CA Cancer J Clin 53: 44-55.
Gluecker, TM and Fletcher, JG (2002). CT colonography (virtual colonoscopy) for the detection
Pickhardt, PJ, Choi, JR, Hwang, I, Butler, JA, et al.
of colorectal polyps and neoplasms. current status and
(2003). Computed tomographic virtual colonoscopy to
future developments. Eur J Cancer 38: 2070-8.
screen for colorectal neoplasia in asymptomatic adults.
Gollub, MJ (2002). Virtual colonoscopy. Lancet 360:
Taylor, SA, Halligan, S and Bartram, CI (2003). CT
Colonography: Methods, Pathology and Pitfalls. Clin
Hardcastle, JD, Chamberlain, JO, Robinson, MH, Moss,
SM, Amar, SS, Balfour, TW, James, PD and Mangham,
CM (1996). Randomised controlled trial of faecal-
Zalis, ME, Perumpillichira, J, Del Frate, C and Hahn, PF
occult-blood screening for colorectal cancer, Lancet
(2003). CT colonography: digital subtraction bowel
348:1472-7.
cleansing with mucosal reconstruction initial
Johnson, CD and Dachman, AH (2000). CT colonography: the next colon screening examination?
Radiology 216: 331-41.
Welcome to Massachusetts General Hospital - Department of Radiology
Dopingautoriteit 1 januari 2008 Lijst van toegestane medicijnen bij sportbeoefening januari 2008 Hieronder tref je een lijst aan van veel gebruikte geneesmiddelen die (soms onder bepaalde voorwaarden) zijn toegestaan. De lijst is per “klacht/kwaal” gerangschikt. Als eerste wordt de naam genoemd waaronder het geneesmiddel te koop is; tussen haakjes is de werkzame stof vermeld (maar
Sehr geehrte Damen und Herren, das Ministerium für Ernährung und Ländlichen Raum und die LUBW Landesanstalt für Umwelt, Messungen und Naturschutz Baden-Württemberg senden Ihnen den aktuellen landesweiten PLENUM-Newsletter. Viel Spass bei der Lektüre! PLENUM-Heckengäu: Urkundenübergabe zur zweiten Runde Am Donnerstag, 5.November 2009 war es soweit: Die Landräte der



 Radiology Rounds
Radiology Rounds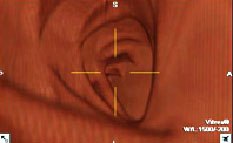
 The present CT colonographic procedure requires
Please note that CT colonography for cancer screening
purgative bowel cleansing with phospho-soda and
is not covered by most insurance at this time. CT
Bisacodyl (Fleet Prep Kit 1) or polyethylene glycol
colonography of asymptomatic patients can be
electrolyte solution (NuLytely® or Go-Lytely®). Prior
performed at MassGeneral West in Waltham or at
to the CT scan, an enema tip or catheter is placed in
the rectum and the colon filled with air until the
patient reports a full feeling. Few patients report any
( Internal Access Only )
The present CT colonographic procedure requires
Please note that CT colonography for cancer screening
purgative bowel cleansing with phospho-soda and
is not covered by most insurance at this time. CT
Bisacodyl (Fleet Prep Kit 1) or polyethylene glycol
colonography of asymptomatic patients can be
electrolyte solution (NuLytely® or Go-Lytely®). Prior
performed at MassGeneral West in Waltham or at
to the CT scan, an enema tip or catheter is placed in
the rectum and the colon filled with air until the
patient reports a full feeling. Few patients report any
( Internal Access Only )