Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Reflexologygr.files.wordpress.com
Comparing the effects of reflexology methods and Ibuprofenadministration on dysmenorrhea in female students of IsfahanUniversity of Medical SciencesMahboubeh Valiani, MSc, Elaheh Babaei, Reza Heshmat, and Zahra Zare, MSc
AbstractBACKGROUND:Dysmenorrhea or menstrual pain is one of the most common disorders experienced by 50% of womenin their reproductive age. Adverse effects of medical treatments and its failure rate of 20-25% have
caused many women to seek other complementary and alternative treatment methods for primarydysmenorrhea. Hence, this study aimed to compare and determine the efficacy of reflexology and
Ibuprofen on reduction of pain intensity and duration of menstrual pain. METHODS:This was a quasi-experimental clinical trial study on 68 students with primary dysmenorrhea living in
Isfahan University of Medical Sciences’ dormitories. Simple random sampling was done considering theinclusion criteria and then the students were randomly divided into two groups. In the reflexology
group, the subjects received 10 reflexology sessions (40 minutes each) in two consecutive mense cycles. The Ibuprofen group received Ibuprofen (400 mg), once every eight hours for 3 days during 3
consecutive mense cycles. To assess the severity of dysmenorrhea, Standard McGill Pain Questionnaire,visual analog scale (VAS) and pain rating index (PRI) were used in this study. RESULTS:Findings of the study showed that the two groups had no statistically significant difference in terms ofdemographic characteristics (p > 0.05). Reflexology method was associated with more reduction of
intensity and duration of menstrual pain in comparison with Ibuprofen therapy. Independent and Paired t-test showed that there was a significant difference in the two groups between intensity and
duration of menstrual pain using VAS and PRI in each of the 3 cycles between reflexology andIbuprofen groups (p < 0.05). CONCLUSIONS:Considering the results of the study, reflexology was superior to Ibuprofen on reducing dysmenorrheaand its treatment effect continued even after discontinuing the intervention in the third cycle.
Therefore, considering that reflexology is a non-invasive, easy and cheap technique, it seems that it canreplace anti-inflammatory drugs (NSAIDs) to avoid their adverse side effects. Keywords: Primary dysmenorrhea, reflexology, ibuprofen, McGill pain questionnaire scale
Dysmenorrhea is a Greek term to describe painful uterine contractions during menstruation and is oneof the most common disorders in women. Dysmenorrhea is the most prevalent problem in women with
different intensities which involves 45 to 95% of women. The prevalence of dysmenorrhea in Iran hasreported as 74 to 86.1 percent.
Dysmenorrhea influences the mental and physical health of women particularly those who are not
seeking healthcare and treatment. It is estimated that annually 140 million work hours and schoolhours are devastated due to symptoms associated with dysmenorrhea and the financial costs of
dysmenorrhea in U.S. is $ 2 billion per year, on the other hand dysmenorrhea causes schoolabsenteeism in 14 to 25 percent of the students. Primary dysmenorrhea is considered as the major
cause of women absenteeism from the work which obviously reduces the quality of life, daily activitiesand economic situation due to decreased working hours, firing from work and increase of health care
costs. There are there therapeutic approaches for the primary dysmenorrhea as the following:
1. Pharmacological approach 2. Non-pharmacological approach 3. Surgical approach. The first-line medical treatment for primary dysmenorrhea is administration of inhibitors of
prostaglandin sysnthesis. These inhibitors should be taken the day before or at the onset of pain andthen every six to eight hours to prevent the formation of prostaglandin byproducts. On the other hand,
consumption of non-steroidal anti-inflammatory drugs (NSAIDs) is prohibited in patients withgastrointestinal problems or those with bronchial sensitivity to aspirin. The side effects of these types of
drugs are nausea, indigestion, diarrhea, fatigue and etc.
Therefore, it seems necessary to provide a non-pharmacological method for such patients who do notrespond to medication or suffer from its side effects and are not willing to consume drugs.
Among these methods, reflexology can be pointed out which is one of the interventions in the manualtherapy groups. Reflexology is not a new method and its history goes back to at least 5000 years ago
in China, India and Egypt. Nearly 2330 years B.C. the primary scientific images of the reflexotherapywas discovered in Ankhmahor's tomb (an Egyptian physician) in Saqqara, Egypt; an image from two
servants who were working on hand and feet of two patients. In this technique, the theory ofassociation between the hands and feet and other parts of the body through the energy lines or
Reflexology is based on the principle that there are reflex areas in the hands and feet which are in
association with muscles, nerves, organs, glands and bones. Specific pressure on specific reflex points
would activate the healing power and make balance in the body. This technique should not bemisinterpreted with massage. Reflexology is a form of pressure which is often done on the feet. Because
feet are the most sensitive parts of the body and that is why they are considered as the best site forimplementing reflexology. Regular reflexology on the body can relieve the anxiety, cause relaxation
Kim and Cho, conducted a study to determine the effects of foot reflexology on premenstrual symptomsand dysmenorrhea in 40 female college students. Mean score of premenstrual symptoms and
dysmenorrhea pain reduced from 8.35 to 4.16 in the first menstrual cycle and to 3.25 in the secondmenstrual cycle by foot reflexology. The results indicated that implementing foot reflexology can be
effective on reducing premenstrual symptoms and dysmenorrhea in female students. Furthermore, astudy by Oleson and Flocco, aimed to determine the effects of ear, hand and foot reflexology on the
premenstrual symptom of 35 women. The results indicated that there was a significant andconsiderable reduction in premenstrual symptoms in those who were in the real reflexology group.
Considering this safe and non-invasive technique (manual therapy) and since reflexology is a noninvasive,
cost effective and a technique with application of hand, it can be well implemented by a skilledmidwife. Due to high prevalence and high loses resulted from dysmenorrhea among the employees
and students and due to reduction of the abilities of women and selecting safer treatment alternatives,the researcher decided to compare the efficacy of this technique with Ibuprofen on reducing the
intensity and duration of dysmenorrhea.
MethodsThis study was a quasi-experimental clinical trial. The study population included all the single female
students living in the dormitories of Isfahan University of Medical Sciences. Eighty people with theprimary dysmenorrhea who were diagnosed by accurate description of their backgrounds and their
families and also checklist, entered the study and were randomly divided into two groups. Treatmentwith Ibuprofen was implemented during three consecutive menstrual cycles and the reflexology group
during two consecutive menstrual cycles. Reflexology was done for 20 daily sessions (40 minutes) onthe study subjects and in the third cycle no reflexology was done in order to compare the durability of
The inclusion criteria included: being single, age range of 18 to 25 years, living in dormitories of IsfahanUniversity of Medical Sciences, suffering from the primary dysmenorrhea with regular menstrual cycles,
the pain should not be associated with non-menstrual pains, lack of endometriosis in one or higher firstgrade relatives, lack of diagnosed chronic diseases (diabetes, high blood pressure, cardiovascular or
pulmonary diseases and etc.) with body mass index (BMI) in the range of 19 to 26, and not employed.
The exclusion criteria included: using pharmacological methods (hormonal and painkiller drugs exceptIbuprofen, herbal drugs) and non-pharmacological methods (such as heat therapy, cryotherapy,
massage and etc.), not participating the reflexology sessions or lack of appropriate Ibuprofen use.
Sampling was done in simple random sampling method considering the inclusion criteria which theywere randomly divided into two groups. Data collection tool was a questionnaire consisted of three
parts; demographic characteristics, menstruation characteristics and dysmenorrhea data, visual analogscale (VAS) and Pain Rating Index (PRI) scales extracted from standard McGill pain scale which was
completed once before the intervention and three times after that by the study subjects.
In the study subjects of reflexology group, by assigning an appropriate time for implementing thetechnique ten days before the probable menstruation time, reflexology was done for 20 minutes on each
foot (totally 40 minutes) in 15 stages generally during two consecutive days (1. Solar plexus, 2 & 3. Areas related to the digestive viscera, 4. Pelvic area, 5. Pituitary, 5. Sinuses, 7. upper and lower
extremities, 8. Spinal cord, 9. Lungs, 10. Shallow chest area [chests], 11 & 12. Back and waist areas, 13. Ovaries, 14. Uterus and 15. Fallopian tubes) and specific reflexology including the areas related to
dysmenorrhea including liver, spleen, the kidneys, pituitary, and the solar plexus. In order toinvestigate and follow-up the durability and lasting effects of reflexology at the third cycle, intervention
was not implemented, but the questionnaire was completed again by the study subjects of this group.
In the Ibuprofen group, in each cycle, a pack of ibuprofen capsules (10 capsules) with the medicationorders (one day before menstruation and the first two days of menstruation, one capsule every 8 hours
after the meal) were given to the study subjects during three consecutive cycles. At the end of eachcycle, the questionnaires were gathered and then the next questionnaire and capsules for the next cycle
were given to them. At the end, the subjects who used drugs irregularly were excluded from the study.
8 subjects from the reflexology group (1 student due to diagnosis of ovarian cysts during theintervention, 4 due to using drugs and 3 due to lack of co-operation) and 4 subjects from the Ibuprofen
group (due to inappropriate use of the drug) were excluded from the study. Finally, 68 subjects (32 inthe reflexology group and 36 subjects in the Ibuprofen group) were left in the study. The collected data
were statistically analyzed using independent and paired t-tests by SPSS software version 16.
ResultsThe mean age of the participants was 21.6 ± 1.79 years (mean ± SD). All the study samples used to take
some techniques to relief their pain and most of them consumed NSAIDs. The BMI of the studysubjects was in the normal range (19-26). Frequency distribution of their academic field of study
showed that most of the participants were educating in sub branches of paramedical science (56subjects or 82.4%) and the rest were educating medical courses (17.6%). In terms of educational degree
of the study subjects, 48 had BS (70.6%), 5 had MSc (7.4%) and the rest had PhD (22.1%). Mean and frequency distribution of menarche age of the study subjects were 13.4 and 1.21 years,
respectively. Comparing the two groups using independent t-test and chi-square test before the
intervention showed no significant difference between the two groups in terms of demographiccharacteristics (age, field of study and degree) and menstrual characteristics (duration of bleeding,
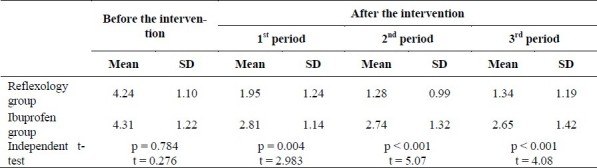
interval between the menstrual periods, rate and volume of bleeding, pain onset and pain site). Mean pain intensity are shown based on VAS and PRI in the reflexology and Ibuprofen groups before
and after the intervention in each of the three menstrual periods. In a comparison which was donebefore and after the intervention in both groups, paired t-test showed that mean pain intensity using
VAS had a significant difference after the intervention in each reflexology and Ibuprofen groups in allthree periods (p < 0.001). These results indicated that mean pain intensity based on VAS in each group
was reduced in comparison with before the intervention. Comparing the two groups in terms of mean intensity of pain with VAS in the first (1), second (2) and
third (3) menstrual periods using independent t-test indicated a significant statistical difference between the two groups with (t = 2.983; p = 0.004) , (t = 5.07; p < 0.001) and (t = 4.08; p <
0.001), respectively (Table 1). Furthermore, comparing the two groups in terms of total score of pain rating index (PRI) after the
intervention in the first, second and third menstrual periods showed a significant difference with (t =2.30; p = 0.024), (t = 3.58; p = 0.001) and (t = 3.89; p < 0.001), respectively (Table 2).
Paired t-test showed that total pain index score before and after the intervention in each reflexologyand Ibuprofen group in each three periods had a significant difference (p < 0.001). These results
indicated that total pain index score had reduced in both groups compared to before the intervention. Moreover, PRI in each of the sensory, emotional, assessment or cognitive and other pains dimensions
were assessed separately. Mean score of sensory pain dimension in McGill questionnaire (with 0 to 42 scores), in the reflexology
group reduced from 17.31 before the intervention to 8.46 after the first menstrual cycle, 6.71 after thesecond cycle and 5.18 after the third cycle. This number also decreased in the Ibuprofen group from
17.38 before the intervention to 12.36, 12.22 and 11.58, respectively. comparing the two groups in termsof sensory pain dimension score through independent t-test before the intervention showed no
significant difference between the two groups (t = 0.04; p = 0.968); however, after the interventioncomparing the two groups in each of the first, second and third periods showed a significant difference
(t = 2.02; p = 0.047) (t = 2.85; p = 0.006) and (t = 3.78; p < 0.001) respectively. Furthermore, in a comparison by paired t-test which was carried out before and after the intervention
in each group, in terms of sensory pain dimension score in each the first, second and third periodsshowed that there was a significant difference between pain intensity before and after the intervention
in each of reflexology and Ibuprofen groups (p < 0.05). Mean score of emotional pain dimension in McGill questionnaire (score 0 to 140), in the reflexology
group reduced from 6.31before the intervention to 2.21 at the first period, 1.59 at the second period and1.09 at the third period. The scores of this dimension in the Ibuprofen group also decreased from 6.91
to 4.19, 3.80 and 3.13 at the first, second and third periods, respectively. Comparing the two groups byindependent t-test before the intervention showed that there was no difference between the two group
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3208937/table/T1/Comparing the mean pain intensity using VAS scale in the study subjects of the both
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3208937/table/T2/Comparing the mean PRI score in the study subjects of the both groups before and
after the intervention in terms of emotional pain dimension score (t = 0.753; p = 0.454), but after the intervention,comparing pain intensity in the emotional dimension showed a significant difference in the two studied
groups in each three menstrual cycles (t = 2.81, p = 0.006) (t = 3.89; p < 0.001) and (t = 3.49; p= 0.001), respectively.
Mean score of cognitive pain dimension in McGill questionnaire (scores 0 to 5) in the reflexology group
was 3.50 before there intervention and reduced to 1.40 at the first period, 1.21 at the second period and1.09 at the third period. In the Ibuprofen group also these scores reduced from 3.05 before the
intervention to 1.75, 2.0 and 1.52 at the first, second and third periods, respectively. Comparing the two groups by independent t-test before the intervention showed that there was no
difference between the groups in terms of cognitive pain dimension score (t = 1.232; p = 0.220), butafter the intervention, comparing pain intensity in the cognitive dimension showed a significant
difference in the two studied groups in each three menstrual cycles as (t = 2.64, p = 0.02) (t = 3.01;p < 0.01) and (t = 3.43; p = 0.008), respectively.
Mean score of other pain dimension in McGill questionnaire (various and different pain dimension,scores 0 to 17) in the reflexology group reduced from 6.84 before the intervention to 3.15 at the first
period, 1.84 at the second period and 1.68 at the third period. The scores of this dimension in theIbuprofen group reduced from 6.83 to 4.41, 4.66 and 4.05 at the first, second and third menstrual
periods, respectively. Comparing the groups by independent t-test before the intervention showed thatthere was no difference between the two groups in terms of other pain dimension score (t = 0.012; p =
0.990), but after the intervention, comparing pain intensity in the other dimension showed a significantdifference in the two studied groups in each three menstrual cycles respectively as (t = 1.78, p =
0.008) (t = 3.91; p < 0.001) and (t = 3.73; p < 0.001). Moreover, in a comparison which was done separately in each group, a significant difference between
the pain intensity in other dimension was indicated at the first, second and third menstrual periods ineach of the reflexology and Ibuprofen groups (paired t-test, p < 0.05).
Mean duration of menstrual pain in the reflexology group reduced from 32.46 hours before theintervention to 15.90 hours at the first period, 14.86 hours at the second period and 9.78 hours at the
third period. In the Ibuprofen group also, mean pain duration reduced from 36.19 hours to 26.19 hoursat the first period, 23.91 hours at the second period and 23.41 hours at the third period.
The results of independent t-test indicated that mean duration of menstrual pain in the two groups hadno difference before the intervention (t = 0.677; p = 0.501). Whereas, after the intervention, both
groups had a significant difference in each three periods in terms of mean duration of menstrual painrespectively as (t = 2.227; p = 0.029) (t = 2.67; p = 0.005) and (t = 2.98; p = 0.004). In a
comparison that was done before and after the intervention in each group, paired t-test showed that ineach first, second and third periods, there was a significant difference between mean duration of
menstrual pain before and after the intervention in each of reflexology and Ibuprofen groups (p <0.05).
DiscussionFindings of the present study showed that intensity and duration of menstrual pain using VAS and PRIand separately by sensory, emotional, cognitive and other pain dimensions in each reflexology and
Ibuprofen groups had a significant difference before and after the intervention. Comparing the two groups showed that reflexology was more effective than Ibuprofen in reducing pain intensity and
Kim and Cho, confirmed the effect of reflexology in relieving menstrual pain. In this study, implementing reflexology on the feet was done for 6 sessions in each menstrual period for two
consecutive cycles. Mean pain score with VAS scale was 8.35 which reduced to 4.16 at the firstmenstruation and 3.25 at the second menstruation after the foot reflexology.
In addition, in the study of Oleson and Flocco, the effect of reflexology was confirmed. In this study,
study subject s randomly were divided into true and false reflexology groups and the results showed asignificant reduction in premenstrual symptoms in the true reflexology group that the durability of the
treatment also remained up to 8 weeks after the intervention (p < 0.001).
In the present study, the effect of reflexology at the second cycle was better than the first cycle; so thatthere was more reduction in mean pain intensity via VAS and PRI.
Many different studies investigated about different complementary medicine methods. In the study of
Wong et al the effect of acupressure on the splenic point VI (SP6) or San Yin Jiao on menstrualdistresses was evaluated. The results indicated a significant reduction in pain intensity score by VAS
scale (p = 0.003) and short form of McGill questionnaire (p = 0.002) immediately after acupressure for20 minutes. The subjects of the acupressure group also statistically showed a significant difference at
the third menstrual period with each one of the scales. It seems that these techniques (acupuncture,acupressure, reflexology and etc.) have more durability than non-steroidal anti-inflammatory drugs such
as Ibuprofen which needs repetition of the drug dosage in each menstrual period. In this regard, Iorno et al in a study titled as “Acupuncture treatment of dysmenorrhea resistant to
conventional medical treatment” on 15 women with mild to severe dysmenorrhea showed that responseto was observed in 13 subjects (87%) and this difference was significant than before the study (p <
0.001). The follow-up of the patients showed that the pain of almost 50% of them had been controlledto six months after the treatment.
Furthermore, the study results of Ghasemi, showed that intensity of dysmenorrhea had a significant
reduction after massage therapy in comparison with before the intervention (p < 0.001). The resultsindicated that the effect of massage therapy on pain intensity was stable even six weeks after the
The results of a study by Aghamiri et al in 2005 titled as “study of effect of acupressure methods onpain in primary dysmenorrhea” on 100 students girls with primary dysmenorrhea in the dormitory
showed that there was a significant difference between mean pain intensity before and after theintervention in the case group (70% reduction). Moreover, the study results showed that there was a
significant difference between mean pain intensity before and after the intervention in the two case andplacebo groups (p < 0.001).
In the present study, the effect of reflexology on reducing the pain intensity influence at the very firstmenstrual cycle and Zhixing also in Traditional Chinese Medicine Hospital (Hangzhou) on 10 women
with dysmenorrhea conducted the foot reflexology and found the immediate effect of reflexology onpain relief in his study samples. Only, three of them did respond to the treatment and required
Suhrabi et al conducted a study titled as “the effect of acupressure in San Yin Jiao point and Ibuprofen
on primary dysmenorrhea” on 80 females college students. Comparing the results showed that painintensity after the treatment at the first and second treatment in both groups had no significant
difference, respectively as (p = 0.073 and p = 0.328), but comparing pain intensity before and after thetreatment in the acupressure group (p < 0.001) and Ibuprofen group (p < 0.001) illustrated a
significant difference. In the present study also, pain duration in each two groups and in each threemenstrual cycles showed a significant reduction.
In addition, comparing the two groups in terms of pain intensity score by independent t-test in eachone of the pain dimensions (sensory, emotional, cognitive and others) showed that the two groups had
no difference in terms of pain intensity score in each sensory, emotional, cognitive and others paindimensions before the intervention, but after the intervention, comparing the two groups in order to
determine the most effective method in each of the first, second and third menstrual cycles, showedthat reflexology group had a better performance than Ibuprofen group (p < 0.05); in other words, this
technique could be more effective in emotional and cognitive dimensions than the pharmacologicalmethod and it had more score reduction in other dimensions.
Perhaps, more reduction of emotional dimension score in the reflexology group was due to more
presence of the researcher along with study samples; i.e. the subjects of this group during this 10 daysof reflexology before incidence of menstruation felt the presence of researcher with themselves and had
more solace, and with expressing their feelings and discharge their emotions could adopt themselvesmore with this physiological phenomenon and maybe due to some reasons such as increase in level of
endogenous endorphins, their pain tolerance threshold had increased more and felt less pain. Therefore, they chosen better words to describe their pain or preferred not to choose a word in some of
the different pain dimensions subsets.
Although the majority of the study subjects in their menstrual cycles used one or more methods toreduce their menstrual pain, the results indicated that duration and intensity of menstrual pain had
reduced in comparison with the time before the intervention.
Overall, this study indicates that implementing reflexology for 20 sessions during the two consecutive cycles, 10 days before menstruation onset could reduce mean intensity and duration of menstrual pain.
Therefore, it can be stated that by conducting more studies about the effect of reflexology on othergroups with primary dysmenorrhea, this technique (which has been highly ignored) can be applied
easily, simple and cost-effectively. Appropriate application of this technique can reduce the menstrual pain in those with primary dysmenorrhea and
consequently reduce medical techniques such as different drugs like painkillers which unconsciously impose some side
Application of different complementary medicine methods such as reflexology technique that does not have any sideeffects similar to chemical drugs and is a simple technique with application of the hands, safer alternatives can be
recommended to treat dysmenorrhea to medical practitioners and those with dysmenorrhea. The authors declare no conflict of interest in this study.
AcknowledgmentsAt the end, our thanks go to Research Deputy of Isfahan University of Medical Sciences and School ofNursing and Midwifery, director of student accommodation and all the students who helped us in
References1. Shah Hosseini Z, Amin GR, Salehi Sormaghi MH, Danesh MM, Abedian K. Double blind study of
anti-primary dysmenorrhea effects of Vitagnus. Journal of Mazandaran University of Medical Sciences. 2006;15(50):15–21. [In Persian]
2. Holtzman DA, Petrocco-Napuli KL, Burke JR. Prospective case series on the effects of lumbosacralmanipulation on dysmenorrhea. J Manipulative Physiol Ther. 2008;31(3):237–46. [PubMed]
3. Dolatian M, Jafari HNV, Afrakhteh M, Taleban FA, Gachkar L. Effects of fish oil on primarydysmenorrhea. Journal of Zanjan University of Medical Sciences. 2004;12(47):7–13. [In Persian]
4. Ehrenthal D, Hoffman M, Hillard PA. Philadelphia: American College of Physicians; 2006. Menstrualdisorders.
5. Arulkumaran S. New Delhi: Jaypee Brothers; 2005. Essentials of gynecology. 6. Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstet Gynecol.
2006;108(2):428–41. [PubMed]7. Berek JS, Novak E. Berek and Novak's gynecology. In: Ghazijahani B, Zonouzi A, Bahrami N,
translators. 14th ed. Tehran: Gholban Arianteb; 2007. [In Persian]8. Quinn F, Hughes CM, Baxter GD. Reflexology in the management of low back pain: a pilot
randomised controlled trial. Complement Ther Med. 2008;16(1):3–8. 9. Wren KR, Norred CL. Philadelphia: Saunders; 2002. Complementary & alternative therapies.
10. Sahai I. Reflexology- A Second Look. 1996. [cited 2011 4 Feb]. Available from:http://www.positivehealth.com/article/reflexology/reflexology-a-second-look .
11. Ebadi MS. Pharmacodynamic basis of herbal medicine. In: Gholami A, Abolhassanzadeh Z,Mohagegzadeh AA, translators. 2nd ed. Tehran: Rahe Kamal: Choghan; 2007. [In Persian]
12. Tiran D, Mack S. Complementary therapies for pregnancy and childbirth. In: Ragaei MA, GoheiriAA, translators. Isfahan Kankash: Isfahan University of Medical Sciences; 2002. [In Persian]
13. Xavier R. Facts on reflexology (foot massage) Nurs J India. 2007;98(1):11–2. [PubMed]14. Kuhn MA. Philadelphia: Lippincott Williams & Wilkins; 1999. Complementary therapies for health
care providers. 15. Wright J. London: Churchill press; 2003. Reflexology and Acupressure: Pressure Points for Healing.
16. Pitman V, MacKenzie K. 2nd ed. Cheltenham: Nelson Thornes; 2002. Reflexology: a practicalapproach.
17. Kim YH, Cho SH. The Effect of Foot Reflexology on Premenstrual Syndrome and Dysmenorrhea inFemale College Students. 2002;8(2):212–21.
18. Oleson T, Flocco W. Randomized controlled study of premenstrual symptoms treated with ear,hand, and foot reflexology. Obstet Gynecol. 1993;82(6):906–11. [PubMed]
19. Blunt E. Integrated healing: Foot Reflexology. Holistic Nursing Practice. 2006;5(6):257–9.
[PubMed]20. Wong CL, Lai KY, Tse HM. Effects of SP6 acupressure on pain and menstrual distress in young
women with dysmenorrhea. Complement Ther Clin Pract. 2010;16(2):64–9. [PubMed]21. Iorno V, Burani R, Bianchini B, Minelli E, Martinelli F, Ciatto S. Acupuncture Treatment of
Dysmenorrhea Resistant to Conventional Medical Treatment. Evid Based Complement Alternat Med. 2008;5(2):227–30. [PMC free article] [PubMed]
22. Ghasemi N. Isfahan: Isfahan University of Medical Sciences; 2008. Effect of massage therapy onpain of endometriosis in women referred to Isfahan infertility center [dissertation] [In Persian]
23. Aghamiri Z, Vigeh M, Latifnezhead RSN. Study of effect of acupressure methods on pain in primarydysmenorrhea. HAYAT. 2005;11(3&4):19–28. [In Persian]
24. Bennett S. Published Research into Reflexology 2011. 2007. [cited 4 Sep]. Available from:www.soothes.co.uk/./reflexology_published_research.pdf .
25. Suhrabi Z, Tadayon M, Javadifar N. Comparison of Pressure Effect on Sanyinjiao Point with that ofIbuprofen on Primary Dysmenorrhea. Journal of Ilam University of Medical Sciences. 2006;14(2):30–5.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3208937http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3208937
15 EPILEPSY AND ANTI- MALARIAL MEDICATION The risk of contracting malaria is high when travelling to some parts of the world, and preventative (or “prophylactic”) medicines are normally recommended to protect the traveller from contracting the infection. It should be noted, however, that these medicines are not 100% effective, and it is important that measures be taken to avoid being
CANADIAN PROSTATE CANCER SUPPORT GROUP Newmarket, Ontario Volume 14, Issue 4, December 15th, 2009 A support group that provides understanding, hope and information to prostate cancer patients and their families Make sure you come to our Christmas Meeting on December 10th, 2009 (note date change, it's the second Thursday this year). At the Newmarket Seniors Meeting Place,
 ResultsThe mean age of the participants was 21.6 ± 1.79 years (mean ± SD). All the study samples used to take
some techniques to relief their pain and most of them consumed NSAIDs. The BMI of the studysubjects was in the normal range (19-26). Frequency distribution of their academic field of study
showed that most of the participants were educating in sub branches of paramedical science (56subjects or 82.4%) and the rest were educating medical courses (17.6%). In terms of educational degree
of the study subjects, 48 had BS (70.6%), 5 had MSc (7.4%) and the rest had PhD (22.1%).
ResultsThe mean age of the participants was 21.6 ± 1.79 years (mean ± SD). All the study samples used to take
some techniques to relief their pain and most of them consumed NSAIDs. The BMI of the studysubjects was in the normal range (19-26). Frequency distribution of their academic field of study
showed that most of the participants were educating in sub branches of paramedical science (56subjects or 82.4%) and the rest were educating medical courses (17.6%). In terms of educational degree
of the study subjects, 48 had BS (70.6%), 5 had MSc (7.4%) and the rest had PhD (22.1%).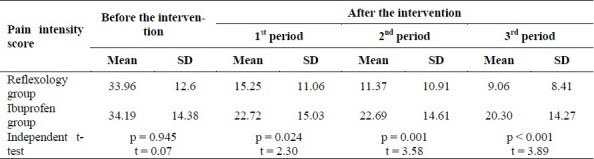 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3208937/table/T2/Comparing the mean PRI score in the study subjects of the both groups before and
after the intervention in terms of emotional pain dimension score (t = 0.753; p = 0.454), but after the intervention,comparing pain intensity in the emotional dimension showed a significant difference in the two studied
groups in each three menstrual cycles (t = 2.81, p = 0.006) (t = 3.89; p < 0.001) and (t = 3.49; p= 0.001), respectively.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3208937/table/T2/Comparing the mean PRI score in the study subjects of the both groups before and
after the intervention in terms of emotional pain dimension score (t = 0.753; p = 0.454), but after the intervention,comparing pain intensity in the emotional dimension showed a significant difference in the two studied
groups in each three menstrual cycles (t = 2.81, p = 0.006) (t = 3.89; p < 0.001) and (t = 3.49; p= 0.001), respectively.