Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Text
INFANTILE COLIC Infantile colic presents in otherwise healthy and well-developing infants as episodes of excessive paroxys-
mal crying, which is not helped by routine comfort measures. Colic begins at about 2 to 3 weeks of age and endsanywhere between 3 and 6 months of age. There is no laboratory test to diagnose colic. Doctors have to rule outall the other conditions that can make the baby cry excessively, some of which can be life-threatening. One of themost widely used definitions, which was proposed by Dr. Wessel back in 1954 (1) and is used by many today,states the "Rule of 3": crying lasting longer than 3 hours per day, 3 days per week and continuing for more than 3weeks. The crying of an infant with colic has a typical pattern described as loud, piercing, high-pitched andaversive. The crying may be accompanied by tensing of the abdominal muscles, flexing of the legs, lifting of thehead, flushing of the face, clenching fingers and passing gas. The peak period of crying usually occurs in theevening. The attack may terminate when the infant is completely exhausted, or with the passage of stool or gas(2).
The estimated number of babies affected by colic published by different researchers varies from as low as
3% to as high as 40%. Most researchers agree the number is somewhere between 10% to 20% (3). With thecurrent birth rate in the United States of about 4,000,000 babies a year, this translates into about 400,000 –800,000 cases of colic a year.The cause, or causes of infantile colic are still unknown. However, doctors who studycolic, have reported many interesting observations:
Colic is more common among the first born (4). Colic is more common among breast fed infants (5). Colici infants have AN increased amount of the hormone motilin in their blood, which is known to stimulate
gastrointestinal tract (Motilin can cause cramping) (6).
Colici infants have an increased amount of serotonin by-products in the urine, suggesting an increased
production of serotonin (Serotonine can also produce cramping) (7).
Colici infants have abnormal contractility of the gallbladder (8)Colici infants have increased intestinal permeability (9). Mothers of colici infants experience more stress and anxiety (10). Mothers of colici infants are older, with higher level of education (5). Mothers of colici infants are more likely to consume broccoli, cauliflower, cabbage, onions, chocolate and
All theories that explain colic fall into several categories: 1. Psychological Psychological, such as an abnormal interaction between mother and infant. One theory suggests that maternal anxiety is sensed by an infant, and an infant responds to such with colic, which in
turn makes the mother more anxious, setting a vicious cycle. Possibly, an anxious mother actually has increasedlevels of yet unidentified substances in her breast milk that cause intestinal cramps in an infant. A combination ofan increased level of maternal anxiety and more frequent breast feedings among the colici infant points towardthis theory. 2. Gastrointestinal Gastrointestinal: hyperactivity, or immaturity of gastrointestinal tract response to either external, or internal
stimulation, intestinal spasms, or excessive production of gas (12, 13, 14). There is a substantial amount ofevidence, such as increased level of motilin, decreased gall bladder activity, and increased hydrogen production,indicating, abnormal function of gastrointestinal tract in colici infants. Gastroesophageal (GE) reflux also has beenproposed as a potential cause of colic. It is true that GE can make the baby cry excessively and simulate colic,however, GE can be successfully treated with either dietary changes, or appropriate anti-reflux medicine. GE is acondition in its own right and should not be confused, or mixed with colic. 3. Allergic disorders Allergic reactions: such as reaction to cow's milk, or other food constituents consumed either by an infant, or
a mother. There is indirect evidence that some infants may suffer from milk protein allergies, or lactose intolerance,or even from general sensitivity to foods consumed by nursing mothers. However, only a minority of colici infantsrespond to hypoallergenic formulas. 4. Misbalance between serotonin and melatonin production. According to this new and intriguing theory, colici infants have increased production of serotonin, which is not
opposed by production of melatonin (15). Production of melatonin normally starts at approximately three monthsof age, when colic frequently ends. Since allergies may be responsible for increased production of serotonin, there
Page 1 of 5
may be a link between the last two theories.
Many different theories try to explain colic. However, none of these theories explains all cases of colic. No
unifying theory takes into account all the known facts of colic. It is likely that colic is a multifactorial condition, whichhas a similar presentation, but is produced by different causes in different infants. USUAL TREATMENT Infantile colic is considered to be one of the most frequent reasons parents seek medical attention for their
children during the first weeks of life. Despite the benign and self-limiting course, infantile colic carries a substan-tial psychological, emotional and physical burden for the parents. Colic can interfere with parent-child bonding,cause strain in a marriage, lead to unnecessary hospitalizations, and in some unfortunate cases, lead to childabuse (16). Mothers of colici babies may experience fantasies of infanticide (17). Unlike previously thought, colicdoes not always disappear without a trace, and some children, who suffered from colic in infancy, may experiencegastrointestinal problems later in their lives (18). Some families may experience abnormal interaction levels aftercolic has ceased (19). Therefore, it is important for health care providers to offer parents of a colici baby, simple,inexpensive and effective medical advice and assistance.
The typical therapeutic interventions for infantile colic offered to parents fall into the 4 categories listed
1. Dietary Dietary manipulations include professional advice on various feeding techniques, or the use of hypoallergenic
milk, soy or lactose free formulas, and an early introduction of solids. (20, 21, 22). However, neither the use of soyformulas, or changes in feeding techniques work effectively. A review of the data studying these recommendationsshowed that use of hypoallergenic formula, such as partially hydrolyzed or amino acid-based, may benefit ap-proximately 25% of infants (23, 24). Occasionally, elimination of offending foods from the maternal diet also mayhelp. 2. Physical Physical strategies include carrying, swaddling, applying abdominal pressure, or massaging the baby. Other
methods include taking an infant for a car ride, use of a car ride stimulator, crib vibrator, or infant swings (25, 26). Another approach is to play recordings of sounds that supposedly soothe the baby. However, a car ride pastmidnight is an extremely impractical method. There is evidence in the medical literature that these methods do notwork (27). 3. Pharmacological Hyoscyamine (levsine™, or gastrosed™) and Dicyclomine are two anticholinergic drugs, (anticholinergic
drugs are similar in their effect to atropine. They dilate pupils, increase heart rate, decrease production of saliva,relieve spasms of gastrointestinal and urinary tracts, as well as bronchi) which are the only prescription medica-tions on the U.S. market that consistently have been shown to effectively treat infantile colic. Unfortunately, up 5%of treated infants may develop side effects, including breathing difficulties, apnea, seizures, syncope, asphyxia,coma and muscular hypotonia (28, 29). In addition, several cases of death have been reported in infants takingdicyclomine (30). It is not surprising that these drugs are rarely prescribed by physician for infantile colic (16,31).Several sedative or sleep-inducing drugs, including diphenhydramine (benadryl™), phenobarbital, chloralhydrate, and even alcohol have been reported as effective treatment for infantile colic. However, there is thepotential for serious side effects associated with these agents, thus limiting their widespread use in treating colic(16, 32). Simethicone (Mylicone), a non-absorbable, over-the-counter drug, which reduces the size of intestinalgas bubbles is frequently recommended, despite several studies that demonstrate the effectiveness of simethiconeon infantile colic is no better than placebo (33, 34).4. Behavioral
Recommendations for behavioral interventions are the most inconsistent therapies available. Some authors
advocate increasing sensory stimulation, while others advocate decreasing such stimulation (16, 31, 35). Otherrecommendations include early response to crying, or allowing THE infant to cry, offering a pacifier, implementa-tion of a routine feeding schedule, using eye contact and interactive playing.
The lack of a safe, effective, practical and affordable therapeutic modality for infantile colic has led many
physicians to believe that counseling, education, reassurance and empathy are the best forms of colic therapyavailable (2, 16, 27). USE OF FENNEL Various plants have been used to relieve of infantile colic, including catmint (Nepeta cataria), chamomille Page 2 of 5
(Matricaria chamomilla), dill (Anethum graveolens), fennel (Foeniculum vulgare), lemon balm (Melissa officinalis),and others. Among these plants, fennel is the most frequently recommended by herbologists and naturopaths. Allof these listed plants are rich in volatile oils, and their beneficial effects are attributed to volatile oils. The highestconcentration of the fennel oil, ranging from 2 to 7%, is found in the seeds. Fennel volatile oil is a mixture of at leasta dozen of different chemicals. The main ingredients of fennel seed oil are: anethole, 40 to 70%; fenchone, 10 to30%; and estragole, 2 to 9%. Other components are present in concentrations usually less than 1%. Animalexperiments have shown that fennel oil regulates contractility of the small intestine (36, 37, 38). Anethole has achemical structure similar to a chemical that is naturally present in the body, called dopamine. Dopamine is knownto have a relaxing effect on the intestine, and perhaps, explains why fennel has a beneficial effect on infantile colic.
Fennel has a long documented history of use, dating to an ancient Egypt. Even today, many lactating moth-
ers in Asian countries routinely take fennel.
Preparations of fennel seed available on the market today exist as either teas or extracts, and contain
variable and unpredictable concentrations of the volatile oil. This variability in oil concentration results from manyfactors, including soil and climate of the growing region, harvesting methods, manufacturing, and storage condi-tions. The inconsistency in the concentration of oil makes it difficult to obtain an effective, predictable and repro-ducible response. That explains why until recently there has only been one clinical study supporting the use ofherbs, including fennel for infantile colic (47). SAFETY OF FENNEL Fennel has the remarkable qualities of being both effective and very safe. No acute or chronic toxic reactions
to fennel, or to fennel products in humans have ever been reported. Laboratory animals given 3000 milligrams offennel extract per kilogram of weight showed no sign of toxicity (39). Likewise, fennel seed oil tested in animalexperiments has been found to be non-toxic at doses significantly higher, than those used in humans. For ex-ample, animals fed a diet containing 1% of anethole, the main component of fennel seed oil, had no toxic effects(40). The recommended daily amount of fennel seed oil for an average colicky 1 month old, who weighs approxi-mately 4 kilograms (9 lbs.), would be 20 to 40 milligrams. Such an infant consumes approximately 600 gram (20oz) of formula, or milk per day. Therefore, 20 to 40 mg. of fennel seed oil given to an infant daily would be equal to0.0035 to 0.007% of the total daily food consumption, which is 140 to 280 times less, than in a study quoted.
Besides its antispasmodic qualities, fennel seed oil has antioxidant and antimicrobial activity, probably attrib-
uted to anethole, which itself has been shown to have anti-inflammatory, antibacterial and also anticarcinogeniceffects (41, 42, 43).
Even though fennel is mentioned as an allergen, the allerginicity of fennel is extremely low, probably much
lower than of milk, soy or eggs. In fact, since 1948 there were only two reports of allergic reaction to fennel plantin the English literature (44, 45). However, all statements of experts regarding the allerginicity of fennel are basedon these two reports. It has been shown that fennel allergy is caused by pollen (46), which is always present inunprocessed seeds. Fennel seed oil, which is produced by distillation of fennel seeds, has no pollen particles in it,and therefore, cannot produce allergic reactions.
Undiluted, or 100% fennel seed oil applied to the skin for a long period of time can produce local irritation.
However, diluted fennel seed oil is not irritating. In an experiment on human volunteers, application of 4% oil didnot produce any reactions.
The Council of Europe included fennel in the list of spices and seasonings in 1973. Fennel seed oil has been
on the FDA's GRAS (Generally Recommended As Safe) list of flavoring substances in the United States since1970's. PEDIACALM After several years of research and study, Lev Laboratories has created uniquely formulated fennel based
• Pediacalm is a stable emulsion of standardized* volatile oil of fennel in water. • Pediacalm is the only standardized herbal dietary supplement for infantile colic. This guarantees the
amount of active ingredients in each bottle.
• Pediacalm is safe, contains no alcohol, bicarbonate or sugar. All ingredients in Pediacalm are FDA
• Pediacalm is the only fennel preparation with patented composition. (US 6 346 250 B2)• Pediacalm is conveniently packaged as a ready to use product into 6 oz nursing bottles. Page 3 of 5
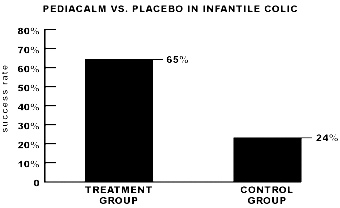
• Pediacalm is effective. This was supported by a recently conducted clinical study. A randomized,
double-blinded, placebo controlled trial, which involved a total of 125 infants demonstrated significant improve-ment (65%) among the infants taking this product in comparison with infants taking placebo (23.7%) (submittedfor publication). BIBLIOGRAPHY 1
Wessel MA, Cobb JC, Jackson EB, Harris GS Jr., Detwiler AC. Paroxysmal fussing in infancy, some-
times called "colic". Pediatrics 1954;14:421-434
Barness LA, Curran JS. The feeding of infants and children. From: Nelson textbook of pediatrics, W. B.
Hide DW, Guyer BM. Prevalence of infantile colic. Arch Dis Child 1982;57:559-60
Ståhlberg M-R. Infantile colic: occurrence and risk factors. Eur J Pediatr 1984;143:108-111
Crocroft NS, Strachan DP. The social origins of infantile colic: questionnaire study covering 76747
Lothe L, Ivarsson S-A, Ekman R, Lindberg T. Motilin and infantile colic. Acta Paediatr Scand
Kurtoglu S, Uzam K, Hallac JK, Coscum A. 5 hydroxy-3-indole acetic acid levels in infantile colic: is
serotoninergic tonus responsible for this problem? Acta Pediatr 1997;86:764-5
Lehtonen L, Svedström E, Korvenranta H. Gallbladder hypocontractility in infantile colic. Acta Paediatr
Lothe L, Lindberg, T, Jacobsson I. Macromolecular adsorption in infants with infantile colic. Acta
Rautava P, Helenius H, Lehtonen L. Psychological predisposing factors for infantile colic.
Lust KD, Brown JE, Thomas W. Maternal intake of cruciferous vegetables and other foods and colic
symptoms in exclusively breast-fed infants. J Am Diet Assoc 1996;96:46-9
Miller JJ, McVeagh P, Fleet GH, Petocz P, Brand JC. Breath hydrogen excretion in infants with colic.
Moore DJ, Robb TA, Davidson GP. Breath hydrogen response to milk containing lactose in colici and
noncolici infants. J Pediatr 1988;113:979-84.
Parmlee AH Jr. Remarks on receiving the C. Anderson Aldrich Award Pediatrics 1977;59:389-395
Weissbluth L, Weissbluth M. Infant colic: the effect of serotonin and melatonin circadian rhythms on
the intestinal smooth muscle. Med Hypotheses 1992;39:164-7
Balon AJ. Management of infantile colic. Amer Pham Physician 1997;55:235-242
Levitsky S, Cooper R. Infant colic syndrome - maternal fantasies of aggression and infanticide. Clin
Iacano G et al. Severe infantile colic and food intolerance: a long-term prospective study. J Pediatr
Page 4 of 5
Canivet C, Jakobsson I, Hagander B. Infantile colic. Follow-up at four years of age: still more "emo-
Lothe L, Lindberg T, Jakobsson, I. Cow’s milk formula as a cause of infantile colic: a double-blind
study. Pediatrics 1982;70:7-10Forsyth BWC. Colic and the effect of changing formulas: a double-blind multiple-crossover study. J Pediatr 1989;115;521-6
Treem WR, Hymas JS, Blackschen E, et al. Evaluation of the effect of a fiber-enriched formula on
Lucassen PLBJ et al. Infantile colic: crying time reduction with a whey hydrolysate: a double-blind,
randomized placebo-controlled trial. Pediatrics 2000;106:1349-54
Estep DC, Kulczycki A, Jr. Treatment of infant colic with amino acid-based infant formula: a prelimi-
Lipton EL. Swaddling and child care practice: historical, cultural and experimental observations.
Byrne JM, Horowitz FD. Rocking as a soothing intervention: the influence of direction and type of
Parkin PC, Schwartz CJ, Manuel BA. Randomized controlled trial of three interventions in the man-
agement of persistent crying of infancy. Pediatrics 1993;92(2):197-201
Williams J, Watkin-Jones R. Dicyclomine: worrying symptoms associated with its use in some small
Myers JH, Moro-Sutherland D, Shook JE. Anticholinergic poisoning in colici infants treated with
hyoscyamine sulfate. Am J Emerg Med 1997;15:532-5
Garriott JC, Rodriguez R, Norton LE. Two cases of death involving dicyclomine in infants. Clinical
Lucassen PLBJ, Assendelft WJJ, Gubbels JW, van Eijk TM, van Geldrop WJ, Effectiveness of treat-
ments for infantile colic: systematic review. BMJ 1998;316(5):1563-9
Gurry D. Infantile colic. Australian Pham Phys 1994;23(3):337-346
Metcalf TJ, Irons TG, Sher LD, et al. Simethicone in the treatment of infant colic: a randomized,
placebo-controlled, multicenter trial. Pediatrics 1994;94:29-34
Danielson B, Hwang CP. Treatment of infantile colic with surface active substance (simethicone). Acta
Carey WB, "Colic" – primary excessive crying as an infant-environmental interaction. Pediatr Clin
North Am 1984;31:993-1005Plant OH, Miller GH. Effects of carminative oils on the muscular activity of thestomach and colon. J Pharmacol Exp Ther 1926;27:149-164.
Imaseki I, Kitabatake Y. Studies on effect of essential oils and their components on the isolated
intestines in mice. Yakugaku Zasshi 1962;82:1326-9
Reiter M, Brandt W. Relaxant Effects on tracheal and ileal smooth muscles of guinea pig. Arzneim.-
Shah AH, Qureshi S, Ageel AM. Toxicity studies in mice of ethanol extracts of Foeniculum vulgare
fruit and Ruta chalepensis aerial parts. J Ethnopharm 1991;34:167-72
Bär F, Gripentrog F. Die Situation in der gesundheitlichen Beurteilung der Aromatisierungsmittel für
Lebensmittel. Madizin Ernähr 1967;5:141-57
Chainy GBN et al. Anethole blocks both early and late cellular responses transduced by tumor
necrosis factor: effect on NF kB, AP-1, JNK, MAPKK and apoptosis. Oncogene 2000;19:2943-50
Ruberto G, Baratta MT, Deans SG, Dorman HJD. Antioxidant and antimicrobial activity of Foeniculum
vulgare and Crithmum maritimum essential oils. Planta Med 2000;66:687-93
Al-Harbi MM et al. Influence of anethole treatment on the tumor induced by Ehrlich ascites carcinoma
cells in paw of Swiss albino mice. Eur J Cancer Prev 1995;4(4):307-18
Levy SB. Bronchial asthma due to ingestion of fennel and fennel seed. Ann Allergy 1948 6:415-6
Schwartz HJ, Jones RT, Rojas AR, Squillace DL, Yunginger JW. Occupational allergic
rhinoconjunctivitis and asthma due to fennel seed. Ann Allergy Asthma Immunol 1997;78:37-40
Jensen-Jarolim E. et al. Characterization of allergens in Apiaceae spices: anise, fennel, coriander
and cumin. Clin Exp Allergy 1997;27:1299-306
Weizman Z, Alkrinawi S, Goldfarb D, Bitran, C. Efficacy of herbal tea preparation in infantile colic. J
Page 5 of 5
TRILYTE (PEG 3350) PREP INSTRUCTIONS FOR YOUR COLONOSCOPY ONE DAY PREP Arrival Date:_____________ Arrival Time:___________Procedure Time: _____________ Endoscopy Center 7 Days Before the Exam: If you are taking Coumadin (Warfarin), Plavix, Lovenox, Aggrenox, Pradaxa, Effient or any other blood thinning medication, make sure you know if and when you are to stop
Congratulations again on your new arrival. We were very happy to be a part of this special time in your life. It is difficult, if not impossible, to set down any hard and fast rules concerning what to do and what not to do when you go home from the hospital. Individuals differ, just as their home and their responsibilities do. However, here is some general information you should know. Vagi
 • Pediacalm is effective. This was supported by a recently conducted clinical study. A randomized,
double-blinded, placebo controlled trial, which involved a total of 125 infants demonstrated significant improve-ment (65%) among the infants taking this product in comparison with infants taking placebo (23.7%) (submittedfor publication).
• Pediacalm is effective. This was supported by a recently conducted clinical study. A randomized,
double-blinded, placebo controlled trial, which involved a total of 125 infants demonstrated significant improve-ment (65%) among the infants taking this product in comparison with infants taking placebo (23.7%) (submittedfor publication).