Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Stroke-isatiii.wikispaces.com
Reduction of Stroke Events With Pravastatin The Prospective Pravastatin Pooling (PPP) Project
Robert P. Byington, PhD; Barry R. Davis, MD, PhD; Jonathan F. Plehn, MD; Harvey D. White, DSc;
Jennifer Baker, MSc, MB; Stuart M. Cobbe, MD; James Shepherd, MD; for the PPP Investigators*
Background—Stroke is a leading cause of death and disability. Although clinical trials of the early lipid-lowering therapies
did not demonstrate a reduction in the rates of stroke, data from recently completed statin trials strongly suggest benefit. Methods and Results—The effect of pravastatin 40 mg/d on stroke events was investigated in a prospectively defined
pooled analysis of 3 large, placebo-controlled, randomized trials that included 19 768 patients with 102 559person-years of follow-up. In all, 598 participants had a stroke during Ϸ5 years of follow-up. The 2 secondaryprevention trials (CARE [Cholesterol And Recurrent Events] and LIPID [Long-term Intervention with Pravastatin inIschemic Disease]) individually demonstrated reductions in nonfatal and total stroke rates. When the 13 173 patientsfrom CARE and LIPID were combined, there was a 22% reduction in total strokes (95% CI 7% to 35%, Pϭ0.01) anda 25% reduction in nonfatal stroke (95% CI 10% to 38%). The beneficial effect of pravastatin on total stroke wasobserved across a wide range of patient characteristics. WOSCOPS (West of Scotland Coronary Prevention Study, aprimary prevention trial in hypercholesterolemic men) exhibited a similar, although smaller, trend for a reduction in totalstroke. Among the CARE/LIPID participants, pravastatin was associated with a 23% reduction in nonhemorrhagicstrokes (95% CI 6% to 37%), but there was no statistical treatment group difference in hemorrhagic or unknown type. Conclusions—Pravastatin reduced the risk of stroke over a wide range of lipid values among patients with documented coronary
disease. This effect was due to a reduction in nonfatal nonhemorrhagic strokes. (Circulation. 2001;103:387-392.) Key Words: lipids Ⅲ prevention Ⅲ stroke Ⅲ trials
Cerebrovascular disease is the second leading cause of
This report presents the results of a pooled analysis of
death in the Americas and Europe, accounting for 10%
stroke data from 3 recently completed event trials that used a
and 14% of all deaths in these regions,1 and is the leading
specific statin, pravastatin. The Prospective Pravastatin Pool-
cause of death among the Western Pacific countries, account-
ing (PPP) Project included data from WOSCOPS (West Of
ing for 14% of all deaths.1 In the United States, strokes killed
Scotland Coronary Prevention Study), the CARE (Cholester-
almost 160 000 persons in 1997 and ranked third as cause of
ol And Recurrent Events) trial, and the LIPID (Long-term
death after heart disease and cancer.2 Approximately 600 000
Intervention with Pravastatin in Ischemic Disease) trial.
persons have a stroke each year in the United States.3 It is a
Individual patient data from the 3 trials were pooled into a
leading cause of disability and increased healthcare costs.3
single database to provide increased power overall and for
subgroup analyses. The larger sample size also permitsanalyses by stroke subtype.
Numerous studies have demonstrated that the risk of
coronary heart disease events is reduced by lipid-loweringtherapy.4–8 The effect of lipid lowering on stroke events is
less well established: meta-analyses of the early clinical trials
The PPP Project was initiated in 1992 before completion of any of
with older lipid-lowering agents have suggested that modest
the constituent trials. The design and rationale for the project havebeen previously described,11 as have been the primary results of the
reductions in cholesterol did not reduce stroke.9,10 However,
3 constituent trials6–8 and the pooled mortality and coronary event
the introduction of the HMG-CoA reductase inhibitors (or
subgroup results.12,13 Each of the 3 studies was a randomized,
“statins”) raised the expectation that these agents might
double-masked, placebo-controlled trial of 40 mg/d pravastatin.
demonstrate a beneficial effect on stroke.
WOSCOPS, conducted in Scotland, was a primary prevention trial
Received June 6, 2000; revision received August 15, 2000; accepted September 8, 2000. From the Wake Forest University School of Medicine (R.P.B.), Winston-Salem, NC; University of Texas School of Public Health (B.R.D.), Houston;
St Francis Hospital (J.F.P.), Roslyn, NY; Green Lane Hospital (H.D.W.), Auckland, New Zealand; Therapeutic Goods Administration (J.B.), Canberra,Australia; and University of Glasgow (S.M.C., J.S.), Glasgow, Scotland.
Guest Editor for this article was Paul M. Ridker, MD, MPH, Brigham and Women’s Hospital, Boston, Mass. Dr Shepherd serves as a consultant to Bristol-Myers Squibb. Dr Byington has an ad hoc consultancy arrangement with Bristol-Myers Squibb. *A complete list of the Prospective Pravastatin Pooling Project Investigators is given in the Appendix. Correspondence to Robert P. Byington, PhD, Department of Public Health Sciences, Wake Forest University School of Medicine, Winston-Salem, NC
2001 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org 387 388 Circulation January 23, 2001 Baseline Descriptions
BP indicates blood pressure; LDL-C, LDL cholesterol; HDL-C, HDL cholesterol; NA, not available. *Includes -blockers, calcium channel blockers, ACE inhibitors, and diuretics.
that evaluated the effectiveness of pravastatin in the prevention of
CARE and LIPID were categorized in the pooled database as
fatal and nonfatal coronary events in 6595 men aged 45 to 64 years
hemorrhagic, nonhemorrhagic, and unknown.
with hyperlipidemia and no history of myocardial infarction (MI).6
Following the PPP protocol, the specific objectives for the
WOSCOPS patients were followed for a mean of 4.8 years. CARE,
analyses presented here were to determine the effect of pravastatin
conducted in the United States and Canada, was a secondary
on the rate of total stroke both for the 3 trials combined and for the
prevention trial that evaluated the effectiveness of pravastatin in the
combination of CARE and LIPID. Analyses of time to first event
prevention of fatal and nonfatal coronary events in 4159 men and
were performed using log-rank statistics and proportional hazards
women aged 21 to 75 years with average lipid levels and an MI 3 to
models.16 In the pooled analyses, tests were stratified by trial. The
20 months before randomization.7 CARE patients were followed for
absolute event rates presented in the tables used the mean follow-up
a mean of 4.8 years. LIPID, conducted in Australia and New
as the unit of time. Interactions between treatment and baseline
Zealand, was also a secondary prevention trial. It evaluated the
characteristics were explored in stratified analyses and proportional
effectiveness of pravastatin in the prevention of coronary deaths in
hazard models. Simple tests of proportions and means were con-
9014 men and women aged 31 to 75 years with a history of MI or
ducted to evaluate treatment group differences in baseline character-
unstable angina and a wider lipid range than CARE.8 LIPID patients
istics. All analyses followed the intention-to-treat principle. Hazard
were followed for a mean of 6.1 years.
ratios and 95% CIs are presented as indications of relative effect
Strokes in WOSCOPS were monitored with national computer-
ized record linking,6 reviewed by an adverse events committee, anddefined as episodes of motor paralysis, sensory or speech dysfunc-
tion, diplopia, or visual disturbance lasting Ͼ1 hour. CARE and
The baseline descriptions of the 3 trials and the treatment
LIPID used an end points committee to predefine and blindly classify
group comparisons are presented in Table 1. Collectively,
strokes. Stroke was defined as a new acute disturbance of focalneurological or monocular function that resulted in either death or
there were 19 768 patients in the PPP database with 102 559
signs and/or symptoms of presumed vascular origin.14,15 Strokes for
Byington et al Pravastatin and Stroke 389 Effect of Pravastatin on Stroke Events
*From proportional hazards model. †From log-rank model, reported only for “total stroke.”
The effects of pravastatin on all stroke events occurring
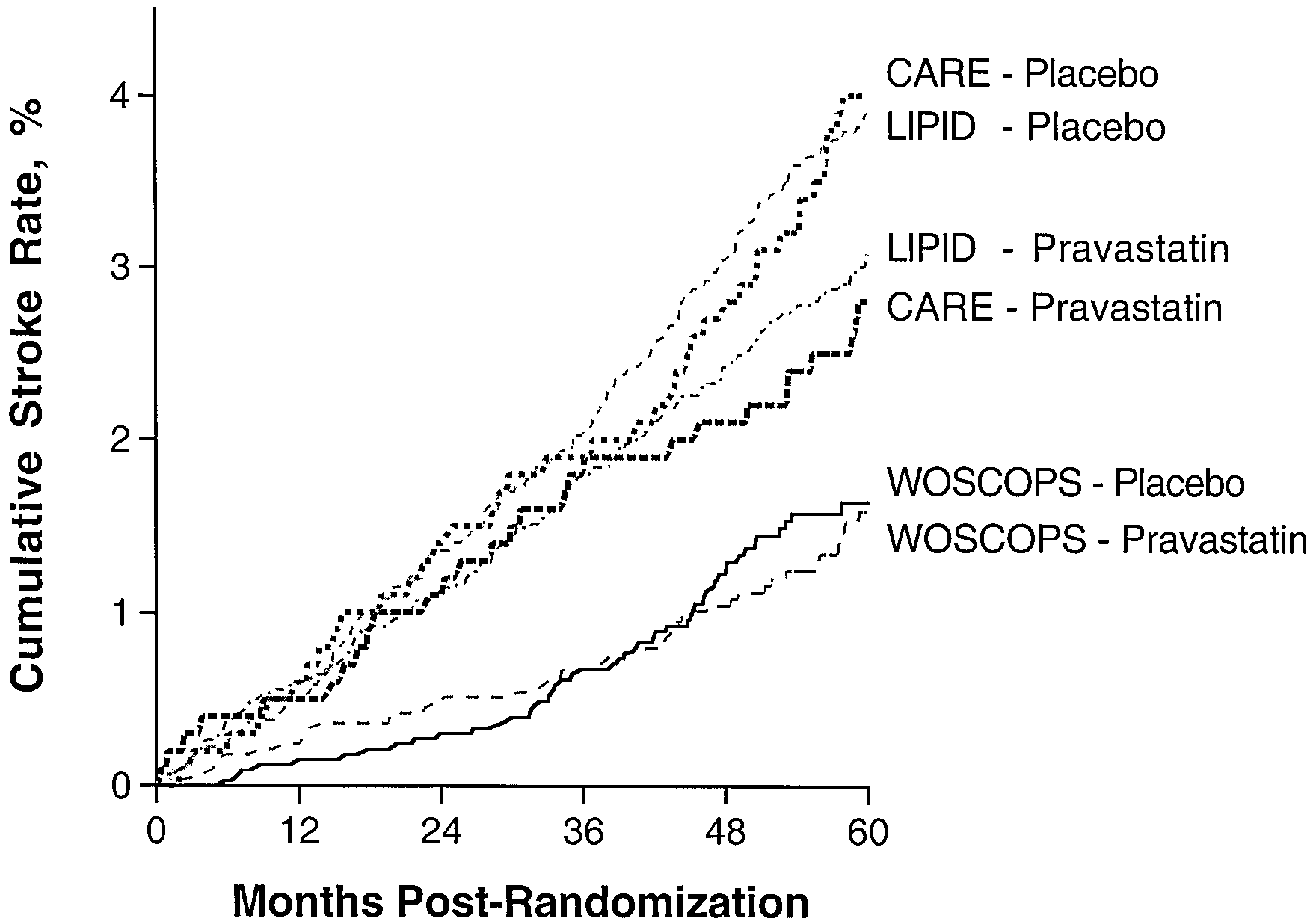
no clear overall benefit attributable to pravastatin. Among the
during the entire follow-up period are presented in Table 2.
2 secondary prevention trials (CARE and LIPID), the stroke
Overall, 598 of the participants had a fatal or nonfatal stroke
rates were generally consistent, both in terms of the long-term
during follow-up. More than half of these were from LIPID,
absolute risks of stroke and the benefit attributable to prava-
although LIPID and CARE had similar placebo group event
statin. Figure 2 presents the cumulative treatment-specific
rates (8.0 and 7.6 strokes ⅐ 1000 patientsϪ1 ⅐ yϪ1, respectively).
stroke curves for the combined CARE and LIPID population,
WOSCOPS had the fewest strokes and the lowest rate of
in which it is noted that the curves diverge after 1 year of
strokes. Each trial individually demonstrated a reduction in
total stroke, although the CI for the WOSCOPS hazard ratio
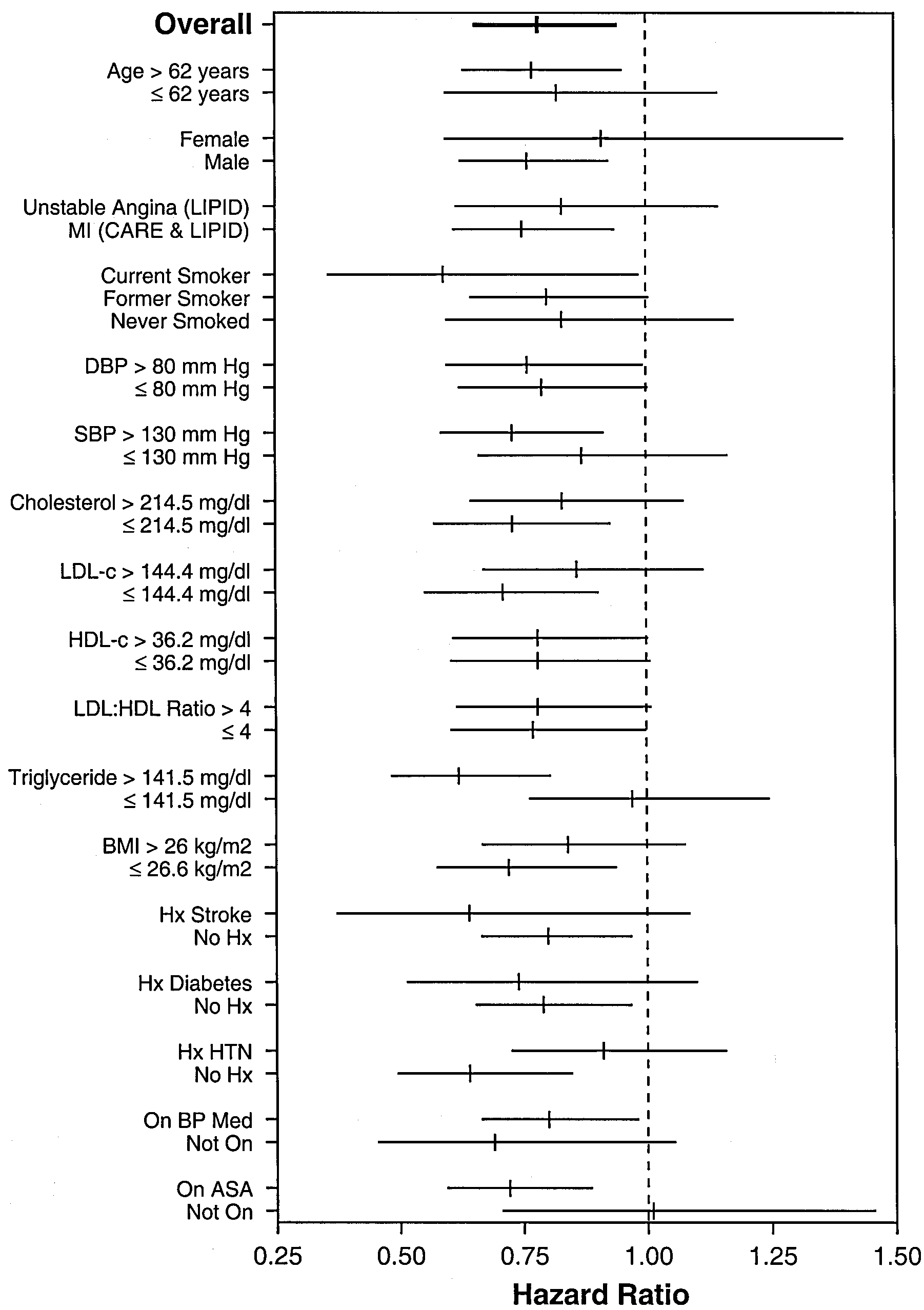
The effect of pravastatin on total stroke was examined in
was large and crossed 1.00 (Table 2, top). CARE had a 32%
various baseline subgroups in the combined CARE/LIPID
reduction (4% to 52% reduction) and LIPID had an 18%
group. The beneficial effect of pravastatin in reducing strokes
reduction (0% to 33% reduction). Combining all 3 trials
was evident and consistent across subgroups (Figure 3).
resulted in a 20% reduction in total stroke with pravastatin
There was no evidence of a statistical interaction (at PϽ0.05)
(7% to 32% reduction, Pϭ0.01). This difference in totalstrokes was maintained if WOSCOPS was removed from thecalculations: CARE and LIPID combined had a 22% reduc-tion (7% to 35% reduction, Pϭ0.01). In the combinedCARE/LIPID database, it was estimated that 588 patientswould have to be treated per year to avert 1 stroke event; inWOSCOPS, 3333 patients would have to be treated.
About 90% of the strokes were nonfatal (Table 2, middle),
and there was an overall 24% reduction in nonfatal strokeattributable to pravastatin. This treatment benefit on nonfatalstrokes was maintained when only the 2 secondary preventiontrials are combined. Less than 10% of the strokes reported inthe trials were fatal (Table 2, bottom).
Figure 1 presents the cumulative fatal/nonfatal stroke
curves. There was no statistical evidence that the proportionalhazards assumption was violated. Event rates in the primary
Figure 1. Occurrence of any stroke (fatal or nonfatal) by clinical
prevention trial (WOSCOPS) were consistently lower, with
390 Circulation January 23, 2001
orrhagic stroke (6% to 37% reduction), primarily a functionof its effect on nonfatal nonhemorrhagic strokes (24% reduc-tion). There is no evidence that pravastatin had an effect onhemorrhagic strokes. Discussion
For decades, there had been considerable doubt regarding thevalue of lipid lowering in stroke prevention. This was becausetotal stroke incidence (in which hemorrhagic and nonhemor-rhagic strokes were combined together) had only been weaklyassociated, if at all, with increased cholesterol levels inobservational studies17 and because of the observed lack ofbenefit of lipid lowering on stroke incidence in the earlycholesterol-lowering trials.9,10 Even as late as 1995, a meta-
Figure 2. Occurrence of any stroke (fatal or nonfatal) by treat-
analysis of cholesterol-lowering trials (none of which used a
ment assignment (CARE and LIPID combined).
statin) reported that patients assigned to cholesterol loweringexperienced no reduction in total stroke.10 In that report,
between any baseline characteristic and treatment group
summarizing the stroke results from 11 randomized trials of
lipid lowering, the relative risk for total fatal/nonfatal stroke
The rates of hemorrhagic and nonhemorrhagic stroke from
in participants assigned to treatment compared with controls
CARE/LIPID are presented in Table 3. Seventy percent of all
stroke events were nonfatal nonhemorrhagic strokes. Prava-
However, this doubt began to evaporate with the publica-
statin was associated with a 23% reduction in total nonhem-
tion of the results of the secondary prevention statin tri-als.18–21 For example, the Scandinavian Simvastatin SurvivalStudy reported in 1995 the post hoc finding that there was a30% reduction in any cerebrovascular event attributable tosimvastatin.22 In another post hoc analysis that same year, apooled analysis of 4 regression trials conducted primarily incoronary patients reported a 62% lower rate of total strokeattributable to pravastatin (Pϭ0.054).4 Subsequently, andwith stroke as a prespecified outcome, CARE and LIPIDindividually reported fewer strokes among patients assignedto pravastatin therapy compared with placebo.7,8 CARE andLIPID remain the only trials to publish the results ofprospectively defined stroke end points. Supporting thesefindings were the results from the B-mode ultrasound regres-sion trials that documented the effectiveness of pravastatin inslowing and/or reversing carotid atherosclerosis.23–25
The analyses presented here clearly demonstrate that prav-
astatin is more effective than the older, nonstatin lipid-lowering therapies in reducing stroke rates. The consistentreductions across the trials and subgroups are striking. Atten-tion is drawn to the beneficial effect of pravastatin amongpatients on aspirin and on or not on blood pressure–loweringmedications. It is also noted that the 22% reduction in relativerisk and the 1.7 ⅐ 1000 patientsϪ1 ⅐ yϪ1 reduction in absoluterisk in CARE/LIPID are comparable to those reported forstroke with antiplatelet therapies given to post-MI patients.26
In observational studies, higher lipid levels have been
associated with higher rates of nonhemorrhagic stroke andlower lipid levels associated with higher rates of hemorrhagic
Figure 3. Effect of pravastatin on total stroke (fatal or nonfatal)
stroke.27,28 Therefore, analyses should be stratified by type of
according to baseline characteristic (95% CIs around hazard
stroke. Moreover, an overall benefit is more likely to be
ratios: CARE/LIPID only). Cholesterol, 214.5 mg/dLϭ5.5 mmol/L;
observed in populations in which nonhemorrhagic strokes
LDL cholesterol (LDL-c), 144.4 mg/dLϭ3.7 mmol/L; HDL choles-terol (HDL-c), 36.2 mg/dLϭ0.9 mmol/L; and triglycerides, 141.5
greatly outnumber hemorrhagic strokes. It has also been
mg/dLϭ1.6 mmol/L. Vertical bar indicates hazard ratio point
estimated from observational studies that hemorrhagic stroke
estimate. DBP indicates diastolic blood pressure; SBP, systolic
rates may increase if the LDL cholesterol levels are Ͻ70
blood pressure; BMI, body mass index; Hx, history of; HTN,
hypertension; BP, blood pressure; Med, medication; and ASA,
Ͻ1.8 mmol/L),21 a level not usually attained with a
40 mg/d dosage of pravastatin. Therefore, the observed PPP
Byington et al Pravastatin and Stroke 391 Effect of Pravastatin on Stroke Type
Data are available for only CARE and LIPID. *From proportional hazards model.
results would be expected: the primary effect of pravastatin
Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344:
were to reduce nonhemorrhagic strokes.
6. Shepherd J, Cobbe SM, Ford I, et al, for the West of Scotland Coronary
The PPP analyses demonstrate that the long-term use of
Prevention Study Group. Prevention of coronary disease with pravastatin
pravastatin is associated with a reduction in total stroke inci-
in men with hypercholesterolemia. N Engl J Med. 1995;333:1301–1307.
dence in the setting of secondary prevention and across a wide
7. Sacks FM, Pfeffer MA, Moye LA, et al, for the Cholesterol and Recurrent
range of patient characteristics. This benefit is seen as a reduc-
Events Trial Investigators. The effect of pravastatin on coronary eventsafter myocardial infarction in patients with average cholesterol levels.
tion in nonfatal nonhemorrhagic strokes. There is a suggestion in
N Engl J Med. 1996;335:1001–1009.
these data that this benefit occurs after Ϸ1 year of therapy.
8. Long-term Intervention with Pravastatin in Ischaemic Disease (LIPID)
Study Group. Prevention of cardiovascular events and death with prava-
Acknowledgment
statin in patients with coronary heart disease and a broad range of initial
The PPP Project is funded by a grant from Bristol-Myers Squibb,
cholesterol levels. N Engl J Med. 1998;339:1349 –1357.
9. Atkins D, Psaty BM, Koepsell TD, et al. Cholesterol reduction and the
risk of stroke in men: a meta-analysis of randomized, controlled trials. Ann Intern Med. 1993;119:136 –145. Appendix
10. Hebert PR, Gaziano JM, Hennekens CH. An overview of trials of cho-
PPP Project Investigators
lesterol lowering and risk of stroke. Arch Intern Med. 1995;155:50 –55.
11. PPP Project Investigators. Design, rationale, and baseline characteristics
Wake Forest University School of Medicine, Winston-Salem, NC:
of the Prospective Pravastatin Pooling (PPP) Project: a combined analysis
Curt D. Furberg, Robert P. Byington, Timothy E. Craven; Brigham
of three large-scale randomized trials: Long-term Intervention with Prav-
& Women’s Hospital, Harvard Medical School, Boston, Mass:
astatin in Ischemic Disease (LIPID), Cholesterol And Recurrent Events
Eugene Braunwald, Marc A. Pfeffer, Frank M. Sacks; University of
(CARE), and West of Scotland Coronary Prevention Study (WOSCOPS). Texas School of Public Health, Houston, Tex: Barry R. Davis, C. Am J Cardiol. 1995;76:899 –905.
Morton Hawkins, Lemuel A. Moyé; National Heart Foundation,
12. Simes J, Braunwald E, Shepherd J, et al, for the PPP Investigators. Victoria, Australia: Andrew Tonkin; University of Sydney, Sydney,
Pravastatin reduces mortality in patients with a broad range of lipid levels
Australia: Anthony C. Keech, R. John Simes; University of Queens-
with or without prior coronary heart disease: the Prospective Pravastatin
land, Herston Old, Australia: Paul Glaziou; University of Glasgow,
Pooling Project. Circulation. 1999;100(suppl I):I-825. Abstract. Glasgow, Scotland: Stuart M. Cobbe, Ian Ford, Christopher J.
13. Sacks FM, Tonkin A, Shepherd J, et al, for the Prospective Pravastatin
Packard, James Shepherd; and Bristol-Myers Squibb Co, Pharma-
Pooling Project Investigators Group. The effect of pravastatin on
ceutical Research Institute, Princeton, NJ (sponsor): Rene Belder,
coronary disease events in subgroups defined by coronary risk factors: the
Sharon Anderson, Kannan Natarajan, Chen-Sheng Lin.
Prospective Pravastatin Pooling Project. Circulation. 2000;102:1893–1900. References
14. Plehn JF, Davis BR, Sacks FM, et al, for the CARE Investigators.
1. World Health Organization. World Health Report 1999 –Making a Dif-
Reduction of stroke incidence after myocardial infarction with prava-
ference. Geneva, Switzerland: World Health Organization; 1999.
statin: the Cholesterol and Recurrent Events (CARE) Study. Circulation.
2. National Center for Health Statistics. Health United States 1999, WithHealth and Aging Chartbook. Hyattsville, Md: National Center for Health
15. White HD, Simes RJ, Anderson NE, et al. Impact of pravastatin therapy
on the risk of stroke: results from the LIPID Study. N Engl J Med. In
3. American Heart Association. 2000 Heart and Stroke Statistical Update.
Dallas, Tex: American Heart Association; 1999.
16. Kalbfleisch JD, Prentice RL. The Statistical Analysis of Failure Time
4. Byington RP, Jukema JW, Salonen JT, et al. Reduction in cardiovascular
Data. New York, NY: John Wiley & Sons Inc; 1980.
events during pravastatin therapy: pooled analysis of clinical events in the
17. Prospective Studies Collaboration. Cholesterol, diastolic blood pressure
Pravastatin Atherosclerosis Intervention Program. Circulation. 1995;92:
and stroke: 13,000 strokes in 450,000 people in 45 prospective cohorts. Lancet. 1995;346:1647–1653.
5. Scandinavian Simvastatin Survival Study Group. Randomised trial of
18. Crouse JR, Byington RP, Hoen HM, et al. Reductase inhibitor mono-
cholesterol lowering in 4444 patients with coronary heart disease: the
therapy and stroke prevention. Arch Intern Med. 1997;157:1305–1310. 392 Circulation January 23, 2001
19. Blauw GJ, Lagaay AM, Smelt AHM, et al. Stroke, statins, and cho-
LDL lowering on atherosclerotic progression in carotid and femoral
lesterol: a meta-analysis of randomized, placebo-controlled, double-blind
arteries. Circulation. 1995;92:1758 –1764.
trials with HMG-CoA reductase inhibitors. Stroke. 1997;28:946 –950.
25. MacMahon S, Sharpe N, Gamble G, et al, on behalf of the LIPID Trial
20. Hebert PR, Gaziano JM, Chan KS, et al. Cholesterol lowering with statin
Research Group. Effects of lowering average or below-average cho-
drugs, risk of stroke, and total mortality. JAMA. 1997;278:313–321.
lesterol levels on the progression of carotid atherosclerosis: results of
21. Crouse JR, Byington RP, Furberg CD. HMG-CoA reductase inhibitor
the LIPID Atherosclerosis Substudy. Circulation. 1998;97:
therapy and stroke reduction: an analysis of clinical trial data. Athero-
26. Antiplatelet Trialists’ Collaboration. Collaborative overview of ran-
22. Kjekshus J, Pedersen TR, for the Scandinavian Simvastatin Survival
domised trials of antiplatelet therapy, I: prevention of death, myocardial
Study Group. Reducing the risk of coronary events: evidence from the
infarction, and stroke by prolonged antiplatelet therapy in various cate-
Scandinavian Simvastatin Survival Group. Am J Cardiol. 1995;76:
gories of patients. Br Med J. 1994;308:81–106.
27. Papadakis JA, Mikhailidis DP, Winder AF. Lipids and stroke: neglect of
23. Crouse JR, Byington RP, Bond MG, et al. Pravastatin, Lipids, and
a useful preventive measure? Cardiovasc Res. 1998;40:265–271.
Atherosclerosis in the Carotid Arteries (PLAC-II). Am J Cardiol. 1995;
28. Iso H, Jacobs DR, Wentworth D, et al, for the MRFIT Research Group.
Serum cholesterol levels and six-year mortality from stroke in 350,977
24. Salonen R, Nyyssönen K, Porkkala E, et al. Kuopio Prevention Study
men screened for the Multiple Risk Factor Intervention Trial. N Engl
(KAPS): a population-based primary prevention trial of the effects of
First in a Series Vaginitis This term describes any infl ammation of the vagina. The most common Although vaginal health concerns cause of infl ammation is infections, but they can also be caused by affect over half of the women in trauma or an allergy to products, such as latex. The most common the United States, many of us infections are yeast infections, bacterial vaginosis
Guidelines for antimicrobial therapy of intra-abdominal infections in adults Infectious Diseases Society of Taiwan; Taiwan Surgical Society of Gastroenterology; Medical Foundation in Memory of Dr. Deh-Lin Cheng; Foundation of Professor Wei-Chuan Hsieh for Infectious Diseases Research and Education; CY Lee’s Research Foundation for Pediatric Infectious Diseases and Vaccines Intra-a
 Byington et al
Byington et al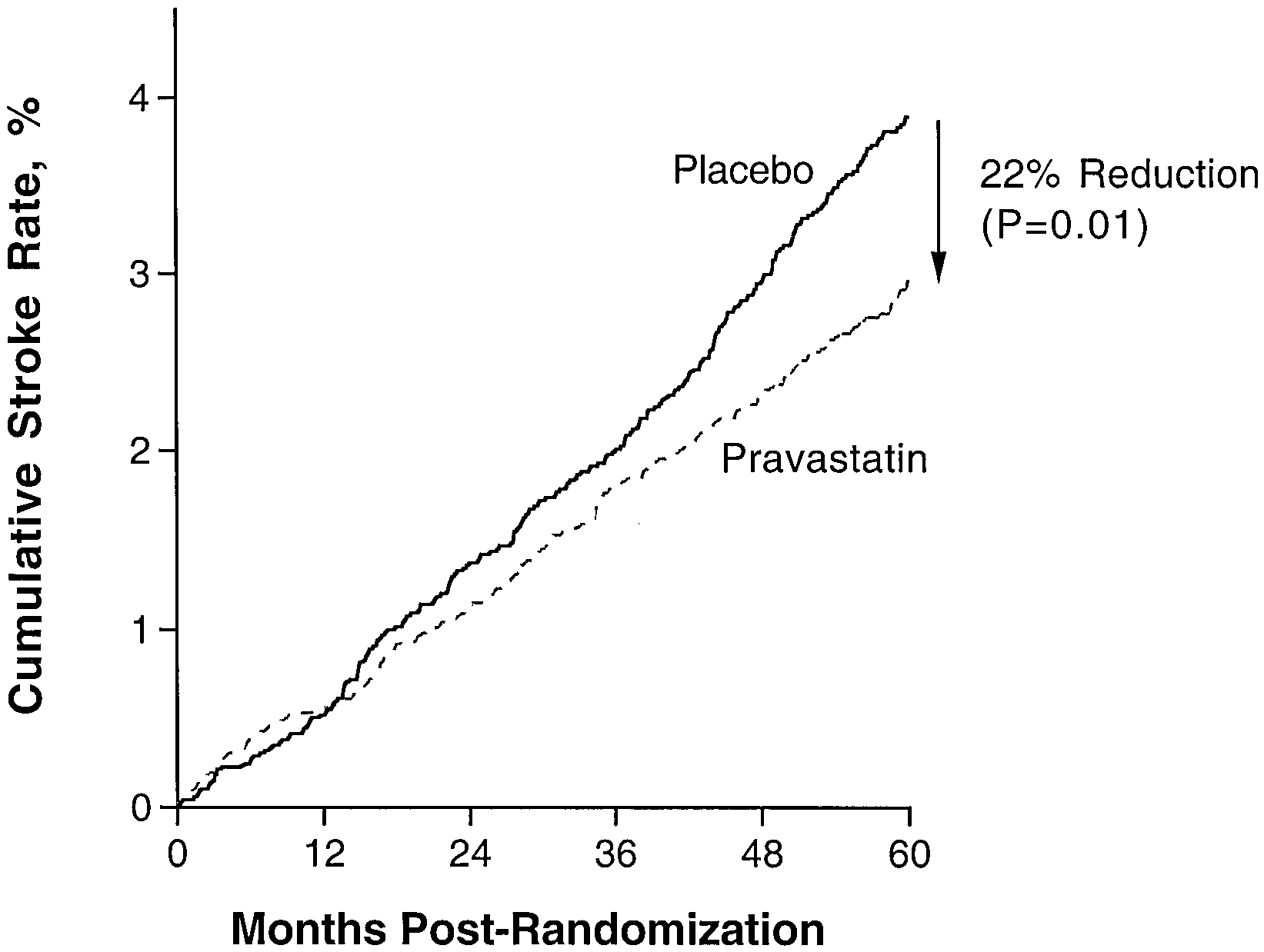
 390
390