Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Aesthetic surgery
The Eye Specialist .co.uk
Age-related macular degeneration (ARMD) Age-related macular degeneration (ARMD) is the commonest cause of blindness in the Western World. Dry ARMD Dry ARMD causes progressive wear and tear of the area of the retina that has the best vision and is untreatable.
Patients often complain of difficulty in reading
newspapers and books, although reading can be easier with a magnifying glass and improved lighting. Sufferers
find it difficult to recognise people’s faces or see the
number on an approaching bus. Treatment of Dry ARMD For Dry ARMD, the treatment options are limited but
include change of lifestyle, improved lighting, training to
use a nondamaged area for vision, low vision / magnifying aids, registration as visually impaired, and
the implantation of an intra-ocular telescope system (the
Intra-Ocular Lens for Visually Impaired People – the IOL-VIP). Although the proof is not conclusive, the AREDS study seems to show that there may be some benefit in taking
oral vitamin supplements as these may slow the
progression of ARMD. There are several commercially
available products, and some of these may be prescribed
on an FP10. The vitamins need to be taken indefinitely.
A change with spectacles often does not improve the vision, either for distance or near. It can be useful to
undergo an assessment for a low visual aid however.
Low Visual Aids (LVAs) are the mainstay for helping patients with ARMD. Although some high street opticians
provide LVAs, they are invariably available as loans from
the Hospital Ophthalmic / Optometry department. A
number of different powers are trialled by a trained optician, although not all patients are suitable. Patients
need to be well motivated as it takes a lot of training to
use an LVA effectively. Patience is required as only a small part of the reading area is magnified (the size
depends on the power of the LVA – the stronger the
power, then the smaller the area that can be read), and
the LVA needs to be moved across the printed words. Inbuilt lights make the LVA more useful. An overhead
reading lamp is also useful for such patients. Some
patients may benefit from a CCTV system – a hand held
camera is passed over the reading material and the magnified image is seen on a TV screen. As Dry ARMD
may slowly deteriorate, reassessment may be required in
the future. Patients do not become completely blind as
they have residual peripheral vision. Training can help to utilise this peripheral vision.
Even if a cataract is present, patients need to be counselled about the guarded prognosis for visual
improvement with cataract surgery in view of the ARMD.
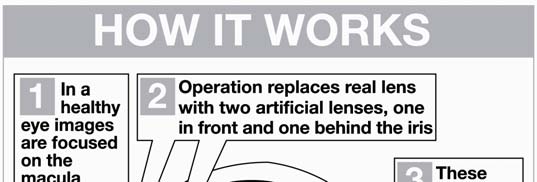
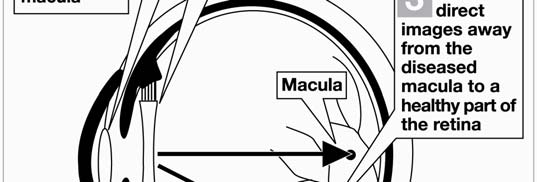
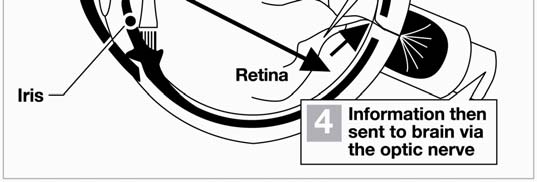
The IOLVIP is a new procedure involving the
implantation of an intraocular telescope which provides
magnification for near tasks in one eye. This acts by
magnifying the image and projecting it via a prismatic lense onto normal retina in another area. Patients
undergo testing for suitability initially, and then training
How the IOLVIP procedure works. (NICE GUIDANCE about IOLVIP -
The new nomenclature for blind registration is the Certificate of Visual Impairment with 2 levels, sight
impaired and severely sight impaired. Although there is
some flexibility on the part of the ophthalmologist, both
the level of vision and amount of central or peripheral visual field loss is taken into account when assessing
eligibility for registration. As a rough guide, patients with
vision of 6/60 or worse are eligible for registration. Where there is extensive field loss e.g. the posterior pole
is scarred from degeneration, or the patient has a
reduced side vision defect following a stroke, registration
can be performed in the presence of reasonable vision if the patient chooses to be registered.
Wet ARMD Wet ARMD accounts for 10% of the disease but 90% of
those patients who are registered as blind. Wet ARMD causes a more sudden visual loss. The
symptoms include loss of vision, visual blur and distortion (e.g. straight lines / door edges appear
Wet ARMD occurs due to abnormal blood vessels under the retina (subretinal neovascular membrane) causing
leakage and build up of fluid and haemorrhage under the
retina, and the retina being lifted off. Ultimately there is
Further investigations (flourescein angiography and
optical coherence tomography) are required to
demonstrate these features and the underlying abnormal
vessels or membrane. Certains types of membrane are
treatable (photodynamic therapy, anti-VEGF injections) depending on the visual level.
Vision testing, flourescein angiography and optical coherence tomography are repeated to assess response
to treatment, and the need for repeat treatments.
Treatment of Wet ARMD
Photodynamic therapy (PDT) is an established treatment
for wet AMD. This involves an intravenous injection of a drug called verterporfin, a photosensitizer which
accumulates in the membrane. Stimulation by non-
thermal red light (laser) causes a reaction which results in damage to the lining of the abnormal blood vessels
and blockage of the leakage. PDT can be supplemented
in some cases with an injection of steroid (triamcinolone)
into the eye. New treatments are targeted towards inhibition of
vascular endothelial growth factor (VEGF) to prevent growth and promote regression of the membrane. Three
agents are in use : Macugen (pegaptanib), Lucentis
(ranibizumab) and Avastin (bevacizumab). All are administered in the form of an intravitreal
injection and are suitable for treating all types of wet
The Eye Specialist .co.uk
Mr S A SADIQ DO MRCOphth FRCS FRCOphth DM
Ahmed’s career
Ahmed qualified from the University of London in 1987, and started training in Ophthalmology in London in 1989. He was a registrar and a fellow in Nottingham, and was appointed as Consultant Ophthalmic Surgeon specialising in phacoemulsification and oculoplastics at the Manchester Royal Eye Hospital in December 1998. He has over 40 publications, more than 40 presentations, and a DM (thesis on endonasal laser DCR). Ahmed’s roles at the Manchester Royal Infirmary & University
Ahmed interviews for the Medical School, and teaches medical and optometry students. He examines medical students, and for the MOptom. He is a member of the Local Negotiating Committee on behalf of the Manchester Royal Eye Hospital, and is a North West Representative of the Hospital Consultants and Specialists Association. He has raised money for the New Children’s Hospital by arranging sponsored events. Ahmed has drafted a new mobile telephone use policy for the Trust which will become part of the hospital’s policies. Ahmed’s roles outside CMMC Ahmed is a nominated representative of the Royal College of Ophthalmologists (RCOphth) on the General Optical Council (GOC). He is a Member of The RCOphth and a Founder Member of The British Oculoplastic Surgery Society. He is an examiner for the RCOphth as well as part of the Training The Trainers and Microsurgical Skills faculties. He has an interest in facial palsy management and is a medical adviser to the British Acoustic Neuroma association. He used to work as an Ophthalmic Medical Practitioner whilst a registrar, is a member of the Ophthalmic Qualifications Committee of the British Medical Association, and is involved with the Education Visitor Panel of the GOC. He is active in research, a journal editor and reviewer. He is a committee member of the British International Doctors Association. He is a medical member of the Appeal Panel of The Postgraduate Medical Training and Education Board. As well as a journal reviewer, he is a reviewer for Research for Patient Benefit and Map of Medicine. Outside medicine, Ahmed is a school governor, is involved with medical charities and community finance initiatives, and is co-chair of the Manchester Christian-Muslim Forum.
The Alexandra Hospital Mill Lane Cheadle Cheshire SK8 2PX t
e [email protected] w www.TheEyeSpecialist.co.uk
Abstracts of the 9th World Congress of Biological Psychiatry PSyChOTiC diSOrderS - Poster Presentations methods: 39 patients (17 female, 12 male, average age 24,8 years) di- p-06-018 agnosed initials with FE and after one year with schizophrenia according parametric variation in working memory demand in patients with DSM-IV criteria were five years of psychiatric (PANSS,CGI-S, CGI-
Joseph Muscarella Jr. Objective I’m seeking the opportunity to become part of a team where the best of my professional experience, and creative skills can be leveraged daily to deliver on the bottom line. I would love the opportunity to continue seeing my designs spread around the world. Experience Personal strong points • Brainstorming fresh, new ideas. • Seeing project

 The Eye Specialist .co.uk
The Eye Specialist .co.uk 
 patients may benefit from a CCTV system – a hand held
camera is passed over the reading material and the magnified image is seen on a TV screen. As Dry ARMD
may slowly deteriorate, reassessment may be required in
the future. Patients do not become completely blind as
they have residual peripheral vision. Training can help to utilise this peripheral vision.
Even if a cataract is present, patients need to be counselled about the guarded prognosis for visual
improvement with cataract surgery in view of the ARMD.
The IOLVIP is a new procedure involving the
implantation of an intraocular telescope which provides
magnification for near tasks in one eye. This acts by
magnifying the image and projecting it via a prismatic lense onto normal retina in another area. Patients
undergo testing for suitability initially, and then training
How the IOLVIP procedure works. (NICE GUIDANCE about IOLVIP -
The new nomenclature for blind registration is the Certificate of Visual Impairment with 2 levels, sight
impaired and severely sight impaired. Although there is
some flexibility on the part of the ophthalmologist, both
the level of vision and amount of central or peripheral visual field loss is taken into account when assessing
eligibility for registration. As a rough guide, patients with
vision of 6/60 or worse are eligible for registration. Where there is extensive field loss e.g. the posterior pole
is scarred from degeneration, or the patient has a
patients may benefit from a CCTV system – a hand held
camera is passed over the reading material and the magnified image is seen on a TV screen. As Dry ARMD
may slowly deteriorate, reassessment may be required in
the future. Patients do not become completely blind as
they have residual peripheral vision. Training can help to utilise this peripheral vision.
Even if a cataract is present, patients need to be counselled about the guarded prognosis for visual
improvement with cataract surgery in view of the ARMD.
The IOLVIP is a new procedure involving the
implantation of an intraocular telescope which provides
magnification for near tasks in one eye. This acts by
magnifying the image and projecting it via a prismatic lense onto normal retina in another area. Patients
undergo testing for suitability initially, and then training
How the IOLVIP procedure works. (NICE GUIDANCE about IOLVIP -
The new nomenclature for blind registration is the Certificate of Visual Impairment with 2 levels, sight
impaired and severely sight impaired. Although there is
some flexibility on the part of the ophthalmologist, both
the level of vision and amount of central or peripheral visual field loss is taken into account when assessing
eligibility for registration. As a rough guide, patients with
vision of 6/60 or worse are eligible for registration. Where there is extensive field loss e.g. the posterior pole
is scarred from degeneration, or the patient has a
 reduced side vision defect following a stroke, registration
can be performed in the presence of reasonable vision if the patient chooses to be registered.
reduced side vision defect following a stroke, registration
can be performed in the presence of reasonable vision if the patient chooses to be registered.

 The Eye Specialist .co.uk
The Eye Specialist .co.uk