Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
Wider research paper 2008-36 the impact of higher standards in patent protection for pharmaceutical industries under the trips agreement: a comparative study of china and india
Research Paper No. 2008/36 The Impact of Higher Standards in Patent Protection for Pharmaceutical Industries under the TRIPS Agreement
A Comparative Study of China and India Xuan Li* April 2008 Abstract
A comparative study is undertaken that explores Chinese and Indian pharmaceutical industries under different patent regimes. It is found that relative to India, which had implemented process patent until 2005, China with a product patent regime since 1993 suffers from both lower drug accessibility and availability (the latter is a missing parameter in the literature). Also, China lags behind in both lower R&D investment and patents filed by Chinese nationals. Based on these findings and associated legal interpretation, we conclude that higher patent protection in China generates negative impacts on the pharmaceutical industries. Thus, governments should utilize TRIPS flexibilities and other regimes like price control to offset the anticompetitive effect in designing patent policies.
Keywords: product patent, process patent, TRIPS, pharmaceutical industries, China, India
This study has been prepared within the UNU-WIDER project on the Southern Engines of Global Growth.
UNU-WIDER acknowledges the financial contributions to the research programme by the governments of Denmark (Royal Ministry of Foreign Affairs), Finland (Ministry for Foreign Affairs), Norway (Royal Ministry of Foreign Affairs), Sweden (Swedish International Development Cooperation Agency—Sida) and the United Kingdom (Department for International Development).
Acknowledgements
The author would like to thank Guanghua Wan, Qin Zhang, Carsten Fink, Ravi Bangar, Christoph Spennemann, and anonymous referees for their helpful comments and suggestions. All views expressed in this paper are the personal views of the author and do not necessarily represent the views of the South Centre or its Member States.
The World Institute for Development Economics Research (WIDER) was established by the United Nations University (UNU) as its first research and training centre and started work in Helsinki, Finland in 1985. The Institute undertakes applied research and policy analysis on structural changes affecting the developing and transitional economies, provides a forum for the advocacy of policies leading to robust, equitable and environmentally sustainable growth, and promotes capacity strengthening and training in the field of economic and social policy making. Work is carried out by staff researchers and visiting scholars in Helsinki and through networks of collaborating scholars and institutions around the world. www.wider.unu.edu [email protected]
UNU World Institute for Development Economics Research (UNU-WIDER) Katajanokanlaituri 6 B, 00160 Helsinki, Finland Typescript prepared by Adam Swallow at UNU-WIDER The views expressed in this publication are those of the author(s). Publication does not imply endorsement by the Institute or the United Nations University, nor by the programme/project sponsors, of any of the views expressed.
1 Introduction
The Agreement on Trade-Related Aspects of Intellectual Property Rights (the TRIPS Agreement) concluded during the Uruguay Round negotiations has led to some changes in the development of pharmaceutical industries. The TRIPS Agreement, which came into effect on 1 January 1995, sets out the minimum standards of protection for all WTO Members. As the TRIPS Agreement implies a substantial increase in terms of patent protection, this paper intends to deal with the following research question: Does a higher standard of patent protection under the TRIPS Agreement have a positive impact on pharmaceutical industries in developing countries?
This paper attempts to compare the welfare effects of patent protection on pharmaceutical industries in China and India respectively. Such a comparison study is possible for two reasons. First, product patent protection for pharmaceuticals has been enforced in China since 1993 (even prior to the introduction of TRIPS to the WTO), which represents one of the longest experiments in setting a higher patent standard protection on pharmaceuticals in developing countries. Second, product patent protection had not been re-implemented in India until 2005, which makes a comparison possible, with presumably a lower patent protection standard on pharmaceuticals.
The structure of this paper is arranged around the central task of illustrating the theme. Following this introduction, Section 2 compares the differences between the key obligations of process patent protection and product patent protection on pharmaceuticals under the TRIPS. Section 3 reviews the literature surrounding the subject matter, while Section 4 compares Chinese and Indian patent patterns and the welfare effects of product patent regimes on pharmaceuticals in China and India respectively. Section 5 presents some interpretations and recommendations, with conclusions drawn in Section 6.
Key issue: process patent protection vs product patent protection
A key legal requirement of the TRIPS Agreement is for all WTO Members to replace process patent with product patent in all fields including pharmaceuticals. Why does the process patent and product patent debate attract considerable attention in the world of pharmaceuticals?
Historically, product patent was excluded in most developed countries. In France, product patent protection was prohibited under the law of 5 July 1844. Since then, French legislation has evolved and limited product patent was allowed on 2 January 1966. In Germany, product patent was explicitly excluded under the law of 25 May 1877 and was introduced as late as 4 September 1967. In Switzerland, product patent for pharmaceuticals was explicitly prohibited by the constitution for a long time and was introduced only in 1977. In Italy, pharmaceutical patents were prohibited until 1978. In Spain, product patent was introduced in 1986 as a consequence of the country’s accession to the European Economic Community (EEC) and the law was effective from 1992 (Boldrin and Levine 2005) (see Figure 1). Likewise, product patent was traditionally excluded in developing countries. Nearly fifty developing countries did not grant patent protection for drugs when the Uruguay Round began in 1986 (Lanjouw
1998). The rationale behind this was to allow local pharmaceutical companies to produce patented drugs by using new processes. Countries may therefore pursue a self-sufficiency policy for the pharmaceutical industry to ensure an adequate supply of medicines at affordable prices to cover the broadest spectrum of diseases (Frischtak 1989).
Technically, a chemical compound (a pharmaceutical product) can be obtained through different processes and methods. From a legal perspective, product patent protection would prevent all other processes and methods from producing the same chemical product. In contrast, under process patent protection, a second producer can produce it provided that an alternative method is used to make the same chemical product.
Economically, a process patent regime promotes a more competitive environment, compared to the monopoly regime created through a product patent. The key lies in the fact that the impact of downstream innovation associated with these two forms of patent protection is substantially different. A process patent would reward the downstream innovator without preventing further innovation while a product patent can prevent further innovation. This issue is particularly important in the area of pharmaceuticals. An inter-industry survey shows that patents are most important to protect innovation within pharmaceutical industries (Levin, et al. 1987). Only five of 130 industries surveyed rated product patents as a method to prevent duplication higher than six (on a seven-point scale) and pharmaceutical industries were one of the five. The explanation for this lies in the unique characteristics of molecules and compounds and the fact that they are extremely easy to copy once discovered (Nogués 1993). In short, a product patent regime increases the patent protection standard significantly comparing to a process patent regime.
Figure 1 Historical evolution on patent regime in selected developed countries
FranceGermany France3 Literature
This section aims to provide an overview concerning the implications of higher standard of patent protection in developing countries. As one of the basic justifications of a patent regime is to foster dynamic innovation as compensation to static losses by granting temporary monopoly rights, the literature review focuses on two dimensions of patent protection: (a) static effects; and (b) dynamic effects.
3.1 Static effects
There is a level of consensus among economists that developing countries will suffer a loss in welfare in the short run with reinforcement of IPRs. Earlier work (Chin and Grossman 1988) suggests that even if IPRs enhance global efficiency for substantial innovations, developing countries would incur important losses and world welfare losses may emerge. Consumers in the developed countries may also suffer from an increase in global prices and other productive inefficiencies if patent protection becomes global (Zuniga and Combe 2002).
Nogues (1993) presents an analytical framework to assess the social losses incurred by the introduction of patent protection for pharmaceuticals. He stresses that the social costs of introducing patent protection depend very much on the pre-patent structure of the pharmaceutical market. This is because patents sustain monopoly prices and if the pre-patent market situation is characterised by competition, the introduction of patents will entail higher social losses than if that situation is characterised by monopolistic behaviour.
Correa (2000) states that static loss is particularly relevant to small countries that rely heavily on technology inflows and lag considerably behind the product cycle. These small economies will find it increasingly difficult to access newly patented inventions if other access or commercialisation incentives are not implemented.
The negative impact of stronger patent protection has been confirmed by several empirical studies. Simulating the introduction of patent protection for pharmaceuticals by assuming different market structures and different demand price elasticities, some studies found non-negligible price increases and welfare losses in southern countries (Nogues 1993; Maskus and Konan 1994; Subramanian 1995). Fink (2000) highlights the importance of available, close and off-patented therapeutic substitute drugs that can restrain prices and limit potential welfare losses.
3.2 Dynamic effects
Contrary to the above consensus regarding negative static effects, the assessment of the dynamic effects of strong patent protection is less categorical. Some theoretical analyses assumed a positive relationship between the strength of patent protection and the rate of innovation. To cite a few examples, according to Kamien and Schwartz (1974), Glibert and Shapira (1990), Klemperer (1990) and Diwan and Rodrick (1991), an increase in patent protection unambiguously promotes innovation.
Diwan and Rodrik (1991) show that if developing countries have a need for innovations that differ from that of developed nations, strong intellectual property protection may be
desirable. Hasper (2005) asserts that IPRs have a positive effect on the health conditions of people in developing countries. Drugs are not available for many diseases that affect developing countries because of weak incentives to manufacture these drugs. Governments of developing countries must negotiate with pharmaceutical firms to obtain these drugs, and stronger IPR protection increases the probability of successful agreements. Weaker IPR protection increases the chances of the drug being copied after it has been introduced, leading to a lower present day value of the drug and lower incentive for drug innovation.
In contrast to the above optimistic views, a number of other studies suggest that there is a significant probability that stronger IPR protection may slow down technological progress in the long run. Chin and Grossman (1990), Deardorff (1992) and Helpman (1993) suggest that mechanistically transferring innovations from the developed world to developing countries is problematic. The spur to domestic innovation is modest in these settings. Segerstrom (1990) suggests that firms still find it profitable to maintain current technologies, to devote fewer resources to or delay investment in development activities and opt to wait longer before marketing a new product or technology. Therefore, extending patent protection to developing countries should not represent a strong stimulus to increase research and development activities; the technology gap separating rich and poor countries may eventually be wider.
The preceding review reveals that the link between strong IPRs and the social welfare impact on pharmaceuticals in developing countries has not been well established. While it is less contentious that patent protection leads to static inefficiency, the dynamic benefits associated with stronger patent protection seem uncertain.
Specifically, some weaknesses can be identified in the existing studies. First, studies on the impact of patents on prices and innovative activity focused almost exclusively on developed economies (Chaudhuri and Goldberg 2003). Second, empirical evidence regarding the impact of the TRIPS Agreement is rather limited. As most developing countries were required to implement the TRIPS in 2005, the actual impact is hard to assess given the limited period of TRIPS implementation. Third, existing studies generally do not differentiate patenting by foreign entities from that by domestic entities in a given country. In view of these limitations, the next section attempts to compare the welfare changes in pharmaceutical industries in China and India respectively under different patent protection standards.
Comparisons between China and India
The potential contribution of a comparative study between China and India rests on two premises. First, there have been contrasting legal settings in terms of patent protection in China and India during 1993-2005, with product patent in China and process patent in India, which makes the comparison of welfare impact between higher and lower standard patent protection possible. Second, there was a similar market structure in the domestic pharmaceutical industry in both China and India prior to the introduction of product patent in China in 1993 (see Figure 2).
Figure 2 Comparison of Chinese and Indian patent regimes
Product Patent China Product Patent India
The first China Patent Law was enacted on 1 April 1985. Only process patent protection was available. Once granted, such a process patent would be valid for 15 years. The first amendment of the Chinese Patent Law came into effect on 1 January, 1993. Under this amendment, product patent may be granted to pharmaceutical compounds used as active ingredients. Product patent may also be granted to chemicals extracted from animals, plants or minerals, provided they have value in pharmaceutical use and are not subject to prior arts. The term of patent protection was extended to 20 years. The 1993 China Patent Law Amendment was generally equivalent to the TRIPS standard introduced in 1995. In comparison, India experienced two major Patent Act amendments, which influenced the pharmaceutical industries’ development path substantially. The Indian Patents Act (1970) introduced process patent to replace the product patent under inherited British colonial law from 1856, which lowered the standard of intellectual property protection substantially in India. The Indian Patent Amendment reintroduced product patent protection to fully implement the TRIPS Agreement commitment, which became effective in 2005. The key commitment is to introduce product patents that were hitherto covered by process patents from 1 January 2005.
Clearly, there were domestic pharmaceutical industries in China and India prior to 1993 when patent protection was introduced. Both countries achieved self-reliant development through reverse engineering. Prior to 1993, the Chinese pharmaceutical industry was characterised by a low degree of concentration: there were a large number of firms with small market shares and a low level of research and development. Similarly, prior to 1970 when the Indian Patent Act was enacted, the Indian pharmaceutical sector was very small (Ramani 2001). From 1970 onwards, Indian pharmaceutical firms slowly eroded the market share of Western companies. The Indian pharmaceuticals sector had been growing from almost nothing before 1970, to a prominent provider of health care products, meeting almost 95 per cent of the country’s pharmaceutical needs (Federation of Indian Chambers of Commerce and Industry 2005). Domestic firms produced about 350 of the 500 bulk drugs consumed in the country in 1993 (Lanjouw 1998). Such a pro-competition pattern prevailed before product patent was re-introduced in 2005. As China and India had similar pharmaceutical drug market structures prior to the introduction of product patent, China and India might have suffered similar static welfare losses.
4.1 Static effects
With the introduction of patent protection, affordability and availability should be two major aspects to be considered when assessing static effects. Currently, while price, which affects affordability, is perceived as the dominant source of the static effect in the literature, little attention has been given to availability. This article covers both aspects.
First, in terms of affordability, this section presents a comparison of selected pharmaceuticals in China and India. One recent case study illustrates the static impact of patents on drugs (Sun 2004). In 2001, for the purpose of monitoring medicine prices and improving access to essential drugs, the World Health Organization (WHO) and Health Action International (HAI) developed a standardised methodology for surveying the availability, affordability and components of medicine prices in developing and transitional countries. Data concerning 14 chronic disease medicines were collected in 30 surveys that covered both China (Shandong Province) and India between 2001 and 2005. To enable international comparison, the price data was expressed as median price ratios (MPR) rather than actual prices, with an international comparison between Chinese prices and international reference prices (WHO and HAI 2005). In the public sector of survey sites in China, the median of the MPR for patented brands (six core medicines) was four times higher than the international reference prices (Management Sciences for Health 2003). About 50 per cent of the patented brand medicines were in the range of 1.71-7.28 times higher than international reference prices. Table 1 summarises the survey results in China. Comparison between the patented brand price and the price of the generic equivalent of ceftriaxone 1 g injection and omeprazole 20 mg tablets illustrates that the median price ratio of the patented brand of ceftriaxone injection was about 18 times higher than that of the lowest generic price found in the clinic facilities surveyed.
Table 1 Summary of median price ratios, public sector, 24 core medicines, Shandong, China
Contrary to China, India has been able to maintain low drug prices, which are among the lowest in the world. For instance, a comparison between a US patented drug and the equivalent Indian drug shows that the US drug price is 40 times higher than that of the generic drug found in India known as Omeprazole. A price comparison of certain blockbuster drugs between US and India is illustrated in Table 2.
Table 2: Blockbuster drugs price comparison of certain drugs in USA and India, US$
Second, in terms of availability, the survey results in Shandong Province, China, demonstrate that the availability of the drugs surveyed was very low in both public and private sectors. Among the core and supplementary medicines in both public and private sectors in survey sites in China, Candesartan, Ciprofloxacin, Co-trimoxazole suspension, Efavirenz, and Stavudine were not found at all. The other eight medicines, namely, Atenolol, Azithromycin, Fluconazole, Ganciclovir inj, Glibenclamide, Lisinopril, Ofloxacin and Olanzapine, whether generics or patented brands, were found in 10 per cent or less of the 40 facilities surveyed.
In the public sector of the survey sites in China, 16 out of the 39 patented brand medicines were found in at least one clinic. Of these, availability across the facilities surveyed was very low, e.g., the highest availability of the patented brand is Diclofenac, which was available in only 45 per cent of the surveyed facilities. In private pharmacy outlets, while 17 patented brands were found in at least one pharmacy, only one patented brand, Diclofenac, was widely available (in 85 per cent of facilities surveyed).
Therefore, the Chinese pharmaceutical market can be characterised as highly priced with very low availability by international standards. In comparison, the Indian pharmaceutical market is comparably more affordable and accessible.
4.2 Dynamic effects
The amount of research and development investment and the number of patents (filing and granted) by nationals are two key indicators to assess the dynamic effects of the patent protection. Though not perfect, these two indicators illustrate to a certain extent the level of inventive activity and the innovative capabilities of a country in a specific sector.
First, in terms of research and development investment, little evidence is found that incentives intended under a higher standard of patent protection after the 1993 Patent Law Amendment have contributed to stimulate Chinese domestic research and development activities.
Chinese domestic pharmaceutical industries spent on average only 0.5 per cent to 3.0 per cent of their turnover on research and development (The Centre for Management of IP in Health R&D 2005). The total amount of research and development expenditure for
Chinese-owned pharmaceuticals was even less than that of a single major Western multinational counterpart. Moreover, rather than undertaking fundamental research work, most of this research and development was oriented towards marketing and commercialisation. Consequently, about 97 per cent of about 3,000 Chinese owned pharmaceuticals produced generic drug versions of foreign brands.
In contrast, Indian research and development expenditure allocated to pharmaceuticals is substantially higher than in China. As the TRIPs Agreement was foreseeable to prevent Indian firms from producing patented drug in 2005, Indian firms accelerated the pace to build up their capacity to innovate. From 2003 to 2004, pharmaceutical industries in India spent approximately 13.2 billion Rupees on research and development; representing 3.6 per cent of their turnover. Chaturvedi and Chataway (2006) suggest that from about 2 per cent of total sales around three to four years ago, the average research and development expenditure of the leading research-based domestic firms in India had gone up to around 5-6 per cent in by 2004. Among these companies, Ranbaxy, Dr Reddy’s, Cipla, Wockhardt, Torrent, Sun, Lupin and Nicholas Piramal are prominent examples. Ranbaxy is among the top 100 pharmaceutical companies in the world and the 15th fastest growing company. It kept a dedicated research facility in Gurgaon staffed with over 1,100 scientists. It spent US$ 75 million on research and development in 2004; a 43 per cent increase over its 2003 expenditure. Dr. Reddy’s research and development expenditure increased from 7 per cent in 2002- 03 to 10 per cent in 2003-04 and was slated to increase further in the future (Chaturvedi and Chataway 2006).
Tables 3 and 4 illustrate that research and development expenditure has been rising and the trend is particularly strong among leading Indian companies, e.g., Ranbaxy, Dr Reddys, and Cipla (Reddy 2006).
In terms of the patent applications, few were filed by Chinese nationals, according to the Invention Patent Bulletin issued by the Chinese State Intellectual Property Office. In the field of chemicals, 91.6 per cent of the patent applications were filed by foreigners, the majority of which were for new chemical synthetic medicines in 2004. In contrast, only a small number of patent applications were filed by Chinese nationals and most of these applications are process patent applications. Differing from the Chinese data, patents filed in India are mainly from domestic Indian firms. Two Indian entities, the Council of Scientific and Industrial Research and Ranbaxy, were in the top ten of the World Intellectual Property Organization’s list in 2002. Patent applications by industry during 1995-2000 indicated that pharmaceutical companies ranked highest with 396 applications. India filed 392 Abbreviated New Drug Applications (ANDA) in 2002. India’s share of ANDA filings has been rising consistently and stood at around 23 per cent in 2003 (Chaturvedi and Chataway 2006).
An important conclusion can be drawn from the above comparisons: in China, while static losses on drugs are certain with poor affordability and availability of drugs, dynamic gains have not been generated with limited research and development expenditure and patent filing by nationals under the higher patent protection standard introduced in China since 1993. Therefore, China has been a loser on both static and dynamic effects with better patent protection. In contrast, India has been able to maintain a good level of drug affordability and availability, as well as promising innovation capacities with lower patent protection.
Table 3 Reported R&D expenditure by Indian pharmaceutical firms, 1991 to 2000
Table 4 R&D expenditure of leading Indian companies
Interpretations and recommendations 5.1 Interpretations
Why does higher patent protection have a negative impact on China’s social system? First, pharmaceutical innovation has a strong cumulative nature. Upstream patents affect follow-on innovations significantly. To illustrate this, it is important to examine how the pharmaceutical industry differs from other industries. The pharmaceutical industry is characterised by the ‘cumulative innovation’ paradigm (Basheer 2005). With this cumulative feature, broad patents, particularly on upstream chemical compound inventions, represent the main threat to competition in the context of the pharmaceutical industry.
The process of creating a new drug is broadly divided into three phases: drug discovery, drug development, and commercialisation. Throughout the entire research and development process, the emphasis is on defining a chemical compound, which is the first but determinant step (Rang 2006). As chemical compound patents stand in the
upstream of the product chain, a broad patent implies that follow-up inventions are dependent on the first patent. Legally speaking, the holder of the upstream patent has the right to exclude others from making, selling or using the invention protected by the patent, as well as preventing others from further research activities and commercially exploiting the invention. Without the authorisation of the first patent owner, a broad upstream patent may block further downstream research and consequently have a negative impact on drug development.
A broad upstream patent is likely to lead its competitors to forgo research and development or refrain from engaging in such activities. Such effects deter market entry and follow-on innovation by competitors and increase the potential for the holders of a board patent to suppress competition (FTC 2003). In China, some multinationals have been exercising the right to prevent Chinese pharmaceutical companies from engaging in downstream innovation activities. To avoid infringing patents, Chinese pharmaceutical companies have to refrain from developing or continuing with a particular innovation that is dependent on the upstream patent.
To sum up, welfare effects differ significantly depending on the patent breadth: a narrow patent (process patent) provides fewer obstacles for follow-up innovation. From a welfare perspective, policy makers should carefully design proper patent breadth to preserve competition, primarily by limiting the scope of patents on upstream inventions.
Further, patent right has a distinct territorial nature. A patent is an exclusive right limited to the territory where it is granted. Thus, national welfare differs significantly depending on the nationality of patent owners. Let’s examine the welfare change by comparing a single-country model and a two-country model. In a single-country model, the nationality of an inventor is indifferent. The transfer of a consumer surplus from consumers to producers (inventors) does not change total welfare, except redistribution.
In a two-country model, however, the welfare analysis is different. Let us assume that there are only two countries in the world; home country H, and foreign country F. Innovation activities are conducted in foreign country F. An inventor from country F is granted a patent in country H. Let us also assume that there was a perfect competitive market in H before inventor from country F was granted a patent in H. In this model, the static effects on country H depend on two factors: first, the size of the deadweight loss, and second, the nationality of the inventor who creates the new product. If newly available patent rights for pharmaceuticals in country H are assigned entirely to inventors from country F, the loss of consumer surplus is a net cost for country H. All of the profits accrue to country F in the form of royalties, if production remains in country H but under licence, or as export profits if the patented drugs are sourced from elsewhere and imported to serve the market in country H (Lanjouw 1998).
In terms of dynamic benefits, where innovation activities take place in this two-country model matters. Such an impact can be differentiated as follows: Unless innovation activities of a newly-granted patent are carried out in the laboratories which the patent owner operates in country H, the dynamic profits of this patent which is supposed to mitigate the static loss for country H are not materialised. The national welfare change in country H is summarised in Table 5. If taking the cumulative nature of the pharmaceutical industry into account, a broad foreign patent would generate more national welfare loss for country H as a broad patent generates a strong negative incentive on follow-up inventions for country H.
Table 5 National welfare change of a foreign patent at H
The above analysis implies that the country of origin of the inventor does affect national welfare. Putting static losses aside, a higher number of domestic patents implies a stronger dynamic profit, whereby a lower number of domestic patents implies a heavier national welfare loss. Given the negative impact on follow-up inventions of a broad upstream patent, the welfare loss in country H would be further aggravated by a broad upstream patent with a foreign country of origin.
5.2 Recommendations
The negative effects of higher patent protection should represent an institutional failure of the TRIPS Agreement. Patents may deter the pace of innovation if patent breadth is not properly designed. Given the minimum standard of protection under the TRIPS Agreement, do national authorities have adequate policy space to pursue an optimal level of patent protection? Two policy options can be considered by developing countries.
First, within the TRIPS Agreement, considerable legal flexibilities still remain for developing countries to pursue their economic objectives in the national context. Patent breadth, patent length and patentability are three major instruments. The degree of market power provided by a patent essentially depends on the combination of these three instruments. While the term of patent protection at 20 years from the date of filing is universal, patent breadth and patentability (height) are two flexible instruments to counter strong market power. For instance, in Japan, narrowly defined patents and promotion of cross-licencing were used effectively to keep drug prices in check while ensuring the introduction of new drugs. While the Japanese system used patent breadth as the main policy instrument to offset overly strong protection, it does not imply that the patentability requirement should be ruled out (Aoki et al. 2006). To demonstrate, adopting stricter patentability criteria is a way to reduce the potentials of blocking patents.
Second, beyond the TRIPS Agreement, policy instruments to offset the blocking effect of patents include competition policy and price control. Competition spurs innovation. Firms may race to be the first to market an innovative technology. Companies may develop lower cost manufacturing processes, thereby increasing their profits and enhancing their ability to compete. Competition can prompt firms to identify consumers’ unmet needs and develop new products to meet those demands (FTC 2003). Drug price control is effective in offsetting the patent effect. The Indian government has
been proactive in defending the country’s interests through the introduction of the Drug Price Control Order. The aim of the 1970 Patent Act was to promote the development of an indigenous pharmaceutical industry and the provision of low-cost access to medicines for Indian consumers. A number of measures introduced including drug price controls, which helped keep Indian pharmaceutical prices low, and boosted the Indian pharmaceutical industry (Chaudhuri and Goldberg 2003).
6 Conclusion
This study shows that a higher standard of patent protection could generate welfare losses for pharmaceutical industries in developing countries. China has been suffering from both static and dynamic losses compared to India, with higher drug prices, lower drug availability and underdeveloped domestic innovation capacity. The comparison is made on two grounds: first, contrasting legal systems in terms of patent protection in China and India, i.e., product patent in China and process patent in India; second, a similar pre-product patent market structure in the domestic pharmaceutical industry in both China and India in 1993. As sufficient flexibilities exist within and beyond the TRIPS Agreement, the governments of developing countries should design socially optimal patent regimes by striking a balance between dynamic gains and static losses.
References
Aoki, R., K. Kensuke and H. Yamane (2006), ‘Indian Patent Policy and Public Health:
Implications from the Japanese Experience’, Discussion Paper 57, Institute of Developing Economics.
Basheer, S. (2005), ‘Block Me Not: Are Patented Genes Essential Facilities?’
University of Oxford, The Berkeley Electronic Press (bepress).
Boldrin, M and D.K. Levine (2005), Against Intellectual Monopoly: The Pharmaceutical Industry, available at: http://www.dklevine.com/general/intellectual/ against.htm, chapter 9.
Chaturvedi, K. and J. Chataway (2006),‘Innovation in the Post-TRIPs Regime in Indian
Pharmaceutical Firms: Implications for Pharmaceutical Innovation Model’.
Chin, J. and G. Grossman (1990) ‘Intellectual Property Rights and North-South Trade’,
in R.W. Jones and A.O. Krueger (eds) The Political Economy of International Trade: Essays in Honor of Robert E. Baldwin (Cambridge, MA: Basil Blackwell) pp. 90-107.
Chin, J. C. and G. M. Grossman (1988), ‘Intellectual Property Rights and North–South
Trade’, NBER Working Paper Series 2769 (Cambridge, MA: National Bureau of Economic Research, November).
Correa, C.M. (2000), International Property Rights, the WTO and Developing Countries. The TRIPS Agreement and Policy Options, London: Zed Books, Third World Network.
Deardorff, A. (1992), ‘Welfare Effects of Global Patent Protection’, Economica, 59, 35-
Diwan, I. and D. Rodrik (1991), ‘Patents, Appropriate Technology, and North-South
Trade’, Journal of International Economics, 63, 79-90.
Federation of Indian Chambers of Commerce and Industry (2005), ‘Competitiveness of
the Indian Pharmaceutical Industry in the New Product Patent Regime’, FICCI Report for National Manufacturing Competitiveness Council.
Fink, C. (2000), ‘How Stronger Patent Protection in India Might Affect the Behavior or
Transnational Pharmaceutical Industries’, Working Paper 2352, Washington DC: World Bank.
Frischtak, C. (1989), ‘The Protection of Intellectual Property Rights and Industrial
Technology Development in Brazil’, Industry and Energy Department Working Paper, Industry Series Paper 13, Washington DC: World Bank.
FTC (2003), ‘To Promote Innovation: The Proper Balance of Competition and Patent
Law and Policy’. Federal Trade Commission.
Gilbert, R., and C. Shapiro (1990), ‘Optimal Patent Length and Breadth’. RAND Journal of Economics, 21, 106-12.
Hasper, M. (2005), ‘Intellectual Property Rights Protections in Developing Countries:
The Effect of TRIPS on the Production and Dissemination of Cures Specific to Developing Country Diseases’, Stanford University, Department of Economics.
Kamien, M.I., and N.L. Schwartz (1974), ‘Patent Life and R&D Rivalry’. American
Klemperer, P. (1990), ‘How Broad Should the Scope of Patent Protection Be?’ RAND Journal of Economics, 21, 113-30.
Lanjouw, J.O. (1998), ‘The Introduction of Pharmaceutical Product Patents in India:
Heartless Exploitation of the Poor and Suffering?’, Working Paper 6366, NBER.
Levin, R.C., A.K. Klevorick, R.R. Nelson, and S.G. Winter (1987), ‘Appropriating the
Returns from Industrial Research and Development’, Brookings Papers on Economic Activity 3.
Maskus, K. and D.E. Konan (1994), ‘Trade-Related Intellectual Property Rights: Issues
and Exploratory Results’, in A. Deardorff and R.M. Stern (eds) Analytical and Negotiating Issues in the Global Trading System (Ann Arbor: University of Michigan Press) pp. 401-46.
Nogués, J.J. (1993), ‘Social Costs and Benefits of Introducing Patent Protection for
Pharmaceutical Drugs in Developing Countries’, The Developing Economies, XXXI-1, 25-39.
Ramani, S. (2002) ‘Who is Interested in Biotech? R&D Strategies, Knowledge Base and
Market Sales of Indian Biopharmaceutical Firms’, Research Policy, 31, 3, 381-98.
Rang, H.P., (2006), Drug Discovery and Development—Technology in Transition,
Segerstrom, P.S., T.C.A. Anant and E. Dinopoulos (1990), ‘A Schumpeterian Model of
the Product Life Cycle’, American Economic Review, American Economic Association, 80, 5, 1077-91.
Subramanian, A. (1994), ‘Putting Some Numbers on the TRIPs Pharmaceutical Debate’,
International Journal of Technology Management. pp. 1-17.
Sun, Q. (2004), ‘A Survey of Medicine Prices, Availability, Affordability and Price
Components in Shandong Province, China’, Center for Health Management and Policy, Shandong University, China.
The Centre for Management of IP in Health R&D (2005), ‘Innovation in Developing
Countries to Meet Health Needs Experiences of Brazil, China, India and South Africa, An overview report to the Commission on Intellectual Property Rights, Innovation and Public Health’, CIPIH.
WHO and HAI (2005), ‘Price, Availability, Affordability: An International Comparison
of Chronic Disease Medicines’, WHO and Health Action International.
Zuniga, M.P. and E. Combe (2002), ‘Introducing Patent Protection in the
Pharmaceutical Section: A First Evaluation on the Mexican Case’, Development, 16, 191-221.
Minutes of the Dorval Elementary School Governing Board Meeting held June 14, 2011, 6:30 p.m. in the staff room. Parents: M. Battaglia, K. Bleakley, L. da Costa, E. Fraser, D. Glavin, B. Pearce, V. Ticknor Staff: C. Arvanitakis, S. Ferrara, C. King, C. Mayer, D. Paiement Community representatives K. Strotmann Regrets: M. Bazinet, C. von Roretz, Public: M. Arciszewska (Preside
INTRODUCCION El Síndrome de ovario poliquístico (SOP) fue inicialmente descripto por Stein y Leventhal en 1935 (1). Es considerado un síndrome, es decir un conjunto de signos y síntomas, en los que un solo test no realiza el diagnostico. Por lo que es necesaria una definición clara y basada en la evidencia debido a las implicancias clínicas que posee esta patología. DEFINICION El

 Research Paper No. 2008/36
Research Paper No. 2008/36 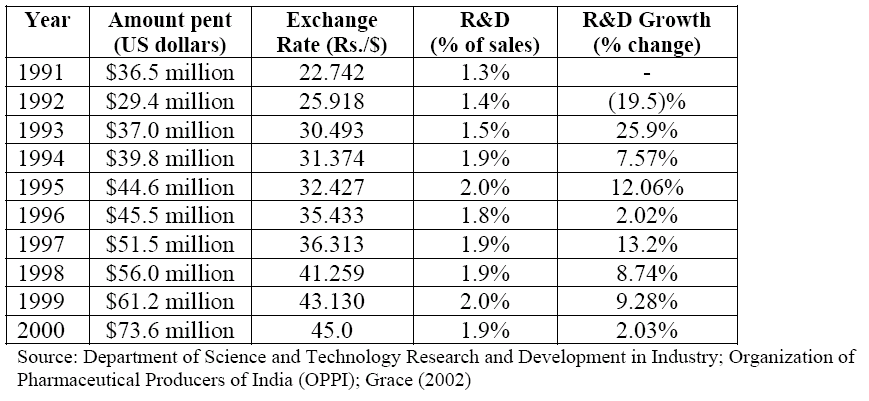
 Table 3 Reported R&D expenditure by Indian pharmaceutical firms, 1991 to 2000
Table 4 R&D expenditure of leading Indian companies
Interpretations and recommendations
Table 3 Reported R&D expenditure by Indian pharmaceutical firms, 1991 to 2000
Table 4 R&D expenditure of leading Indian companies
Interpretations and recommendations