Tadalafil gehört zur Gruppe der PDE5-Hemmer und wirkt über eine hochselektive Blockade des Enzyms Phosphodiesterase Typ 5. Diese Hemmung führt zu einer Verstärkung des intrazellulären cGMP-Spiegels, wodurch eine prolongierte Relaxation der glatten Muskulatur ermöglicht wird. Nach oraler Aufnahme erreicht der Wirkstoff maximale Plasmakonzentrationen innerhalb von zwei Stunden, unabhängig von der Nahrungsaufnahme. Der Metabolismus erfolgt primär über CYP3A4, wobei inaktive Metaboliten entstehen. Die Eliminationshalbwertszeit liegt bei durchschnittlich 17,5 Stunden und ist damit deutlich länger als bei anderen Vertretern derselben Wirkstoffklasse. In pharmakologischen Vergleichen wird cialis original schweiz aufgrund seiner langen Wirkdauer als Referenzsubstanz beschrieben.
response to concerns about piper methysticum forst.f, kava - submitted to mca [pdf]
Response to concerns about Piper methysticum Forst. f., Kava. A submission prepared by the Traditional Medicines Evaluation Committee (TMEC), a subcommittee of the European Herbal Practitioners Association. Submission Date: 11/1/02 Introduction
This submission has been written by TMEC in response to a report recently circulated by theGerman BfArM. This agency has recently advised that there have been a number of adverseevents associated with the use of concentrated standardised preparations of kava reportedfrom Germany and Switzerland.
Kava is a significant herbal medicine with some unique properties and the ability of herbalpractitioners to care for their patients would be seriously affected if its use were restrictedand they were unable to use it. This TMEC submission argues that many of the adverseevents cited by BfArM ought not to be attributed to kava and that, in addition, theproperties of concentrated standardised extracts, as opposed to those preparations whichapproximate to traditional kava use, may be a contributory factor in causing adverseevents. This paper proposes a number of simple measures that will ensure that kava maycontinue to be safely available in the UK. Benefits of Kava Kava has been used in Britain by herbal practitioners since the early 1900’s mainly for urinary problems (Ellingwood, 1919). The indications given in the British Herbal Pharmacopoeia (Anon, 1983) are “Cystitis. Urethritis. Rheumatism. Infection of the genito- urinary tract”. More recent texts emphasize its usage as a nervine. For example, indications given by Mills, Bone (2000) are “anxiety of nervous origin, nervous tension, restlessness or mild depression of non-psychotic origin, menopausal symptoms (Indications supported by clinical trials) “ and “inflammation and infections of the genitourinary tract of both men and women; pain of muscular and nervous origin; insomnia. (Traditional therapeutic uses).” The use of kava as a nervine has increased markedly in recent years partly due to the evidence for effectiveness found in clinical trials (Pittler, Ernst, 2000). However, it is interesting to note that such usage is not completely new. Felter (1905) notes its application, inter alia, in neuralgia, dizziness and despondency. It has a particular value in agitation and anxiety (Spinella, 2001), being useful when other nervines have proved ineffective.
Clinical trials have been reviewed most recently by Pittler & Ernst (2000) who state that fortreating anxiety superiority over placebo was suggested by all seven trials under review andthat, for the three trials included in the meta-analysis, there was a significant reduction inscore on the Hamilton Anxiety Scale. The clinical trials were all carried out in Germanywhere kava is prescribed both by doctors and sold OTC in pharmacies for anxiety andinsomnia. This usage is backed by evidence derived from eight double-blind randomisedclinical trials, involving 663 patients, which are reviewed in the draft submission to BfArM bytwo pharmaceutical associations, the Bundesverband der Arzneimittel Herstell e.V. (BAH)and Bundersverband der Pharmazeutischen Industrie e.V. (BPI) This document refers tothree recent trials which are awaiting publication. These trials have used a range of productsstandardised on 15-70% kava lactones giving a daily dosage of 60 - 210mg daily of kavalactones. The use of kava is being increasingly advocated for use in anxiety as analternative to benzodiazepines. For example, De Leo et al, (2001) showed a significantrelative decrease in anxiety in a double-blind randomised trial on 40 menopausal womenwhen kava was combined with hormone replacement therapy.
The modern use of kava as a nervine is in accordance with its traditional usage in the SouthPacific. Kava drinkers report a sense of relaxation and tranquility and a sociable attitude(Chanwai, 2000). It is used as a social and ceremonial drink amongst men in Polynesia. Inmodern times as the influence of the church decreased, its use has become morewidespread and frequent. Kava is an important part of social life in Fiji for instance. Fijianspiritual leaders are called dauvaguna the literal translation of which means “expert atdrinking kava”. (Greenwood-Robinson, 1999). Kava is said not to be addictive and not toappear to have the violent antisocial effects of use of alcohol (Lebot et al, 1997). However(see below), there are serious concerns in Australia (Clough, et al, 2000) about its abuse asa recreational drug when used to excess. What is kava? Root bark and root of kava are used, either fresh or dried. Based on an archaeological study of the characteristic drinking bowls, it is proposed that it was first domesticated in Polynesia over 2,000 years ago (Green, cited in Lebot et al, 1997). A comprehensive survey by Lebot and Levesque in 1984 (cited by Lebot et al, 1997) suggests that it was originally domesticated in Vanuatu. Kava is now obtained from a range of cultivars in the South Pacific. It is always vegetatively propagated from stem cuttings as it is sterile. There are many cultivars and new strains continue to be developed by Polynesian farmers as each is considered to have different psychoactive effects. In recent years, there has been increasing pressure on the market because of the increased worldwide demand for kava. In 1998, it was amongst the top-selling herbs in the USA with a turnover of eight million dollars representing a growth rate of 473% (Pittler, Ernst, 2000). It is possible that the current hepatotoxity problems are to some extent consequent on poor quality control caused by a rapid and extraordinary increase in the size of the market (Murray, 2000). However since a range of products is implicated, this is unlikely to provide a satisfactory explanation for all the reported adverse reactions. It is to be hoped that the German BfArM will release relevant data about the source and quality assurance of supply in due course. Phamacology Kava is an unusually well-researched herb. The crystalline resin was first isolated in 1857 by a French naval pharmacist and a detailed monograph was published in 1886 (Lewin, cited by Lebot et al, 1997). The kava lactones are considered to be the active constituents and have been shown in animal studies to have a sedative action (Grunze, et al., 2001), although the mechanism is unclear (Spinella, 2001). The kava lactones are found in the resinous portion (5-9%) of the plant material and are thus poorly soluble in water. This fact may have important implications for its safe use (see below
Kava lactones are 4-methoxy-2-pyrones with phenyl or styryl substituents at the 6thposition (Lebot et al, 1997) and are found in the resinous plant material. Total kava lactonecontent varies from 3-20% dry weight and eighteen lactones have so far been isolated (He,et al, 1997) with the following six compounds being considered most important:
chiral enantiomers (Haberlein, et al, 1997) (STRUCTURES)(+)-kavain (+)-dihydrokavain(+)-methysticin (+)-dihydromethysticinachiral dienolides:yangonin demethoxyangonin
Traditional preparation techniques. Kava is traditionally prepared in the South Pacific by grinding and mixing the root or root bark with cold water. This makes an emulsion that is a suspension of the resinous constituents in water (Lebot et al, 1997). It is also prepared as an emulsion (also traditionally prepared without heating) in coconut milk (Johnson, 1999). Modern preparation techniques The bioavailability of kava constituents varies substantially depending on the method of extraction employed (Hansel et al, 1994 cited in Schulz et al, 1997). Kava is predominantly available in Germany as a so-called concentrated standardised extract seemingly designed to maximize extraction of the kava lactones. For these concentrated standardised extracts, Schulz (1997) states that kava is dissolved in a high percentage of ethanol- to-water
mixture to obtain extracts containing about 30% kava lactones or alternatively using anacetone-water mixture to obtain extracts containing about 70% kava lactones. Both typesof product have a herb-to-extract ratio of about 12-20:1 (Schulz, 1997). The dosagerecommended by Commission E is expressed as the equivalent of 60-120mg kava lactonesdaily. A paper by Whitton, Whitehouse and Evans (see Appendix 1) makes the same pointabout enhanced kava-lactone extraction using a high ethanol or acetone medium but detailssomewhat different extraction values.
The preparation methods used for standardised products are highly technical and extractionrates vary (Kubatova, et al, 2001) depending on solvent and temperature. As the paper(Appendix 1) by Whitton et al demonstrates, both efficacy and safety depend on the kavalactones remaining in their natural form and on the extraction of the other naturalconstituents of the plant.
Varying extraction techniques and preparation methods may result in:
• An unnatural variation in the relative concentration of each lactone.
• Artefacts of production which may have a potential hepatotoxic action.
It should be noted that commercial kava products may also contain synthetic racemickavain that may have other characteristics than the naturally occurring product.
It is clear that these technical matters related to extraction techniques require furtherelucidation and we await further data from BfArM and manufacturers of kava products.
Proponents of concentrated standardised products assert that they provide an effective dosewithin a consistent range. The traditional water-based kava preparations of the Polynesianpeoples and low-alcohol kava tinctures employed by herbal practitioners have beenconsidered unreliable because the concentration of active constituents varies from kavabatch to batch. However, there are three relevant counter-arguments:
1. The whole range of the constituents may produce a more effective and safe medicine
which has been demonstrated in kava (Williamson, 2001).
2. Some constituents, not necessarily considered active, may enhance the safety of the
medicine. (See the specific point about glutathione made by Whitton et al in the paper inAppendix 1).
3. Definitive isolation of the active constituent has proved elusive in other medicinal plants
such as Hypericum perforatum (Barnes et al, 2001).
4. Herbal practitioners rely on the synergy between a whole range of constituents in the
herb(s) within a herbal prescription which is individually prescribed for the patient. Thispositive interaction also has the benefit of keeping levels of any one constituent belowthe safety threshold. The advantages of low alcohol tinctures TMEC strongly advocates the employment of extraction techniques which closely resemble those traditionally used in Polynesia. This would require the use of low-alcohol tinctures made by the traditional cold maceration processes common to UK tincture making. (Evidence for the safety implications of such tinctures is set out in detail in the paper by Whitton et al. See Appendix 1). The reasons for this opinion are set out below. Tinctures used by herbal practitioners are prepared by macerating dry kava in a mixture of water and ethanol. It has been shown that such extracts using 25% ethanol /75% water contain up to 30 times less lactones that the concentrated standardised preparations (See Appendix 1). The traditional preparation method in a mixture of 25% ethanol/water extracts a much wider range of the natural kava constituents, Whitton et al (2002). Whitton et al (2002) have also reported the presence of glutathione in kava which is likely to be important in the metabolism of kava lactones in the liver, reducing any chance of potential toxicity. The same authors have demonstrated that the glutathione present in the plant is not extracted in high-alcohol or high-acetone extracts. In the cases of alleged toxicity due to kava, there are instances where concomitant use of drugs or alcohol are likely to have
depleted the reserve of glutathione in hepatocytes. This may predispose the individual tosensitivity to kava products with high kava lactone concentrations such as are found instandardised extracts, particularly when such an individual is also taking an orthodoxmedicine that may itself put pressure on the liver. On the other hand, not only would thekava lactones in the traditional extract be at lower concentration, but the glutathionepresent in the extract may allow the kava lactones to be metabolised in the liver even inconditions of glutathione depletion. This may explain the absence of kava toxicity fromtraditional preparations which have been used extensively and long-term even at highconcentrations. In addition, research by Whitton et al currently in progress (See Appendix1) proposes that low ethanol extracts of kava contain glutathione which may have ahepatoprotective effect if the person is, for any reason, in danger of saturation of thehepatic enzymatic detoxification pathways (see below). Dosage Assuming a 1:5 25% tincture and an upper limit of 20% lactones in the dried herb (concentrations stated as 3-20%, see section on Pharmacology, page 2), then 500 ml would contain (100 x 0.2 x 0.15) = 3 g (3000 mg) of kava lactones. Further assuming a daily dosage of 5-10ml of the 1:5 25% tincture, the daily dose of kava lactones amounts to a maximum of 30-60mg. If the concentration of kava lactones were lower, e.g. at around 10% as appears to be the case with regard to Australian kava discussed by Clough et al. (2000), then this figure falls to 15 –30 mg per day. It is noteworthy that the maximum daily dosage here is equivalent to the minimum daily dosages of the 60-210 mg kava lactones given in clinical trials of kava conducted in Germany.
Although standardised extracts provide a higher dosage of kava lactones than low-alcoholtinctures, over-dosage in itself is unlikely to be the cause of hepatotoxicity. Strong evidencefor this is the fact that kava is taken daily at high doses as a normal part of daily life inlarge areas of the South Pacific. Indeed, some of the accounts of high kava intake areremarkable. For example Chanwai (2000) describes the case of a man who was admitted tocasualty after an overdose but slept off his symptoms, who admitted to consuming up to 40bowls a day for the last 14 years. In Australia, missionaries introduced kava to theaborigines in the 1980s as a substitute for alcohol. Since that time kava has been abusedlike alcohol and it is claimed that many people consume as much as fifty times the amounttypically drunk by South Pacific islanders (Green-Wood-Robinson, 1999). Clough et al(2000) discuss concern over heavy usage of kava in Australia and describe normal use ofkava in the Northern Territory as 37g of kava powder (containing around 3800 mg of kavalactones) per hour with heavy consumers using around 610g weekly prepared as a drink. The incidence of serious illness resulting from hepatotoxicity associated with regular kavausage would surely have been observed by the medical services in Polynesia and Australia ifover-dosage of lactones were the main cause of hepatotoxicity.
There is a justified concern in Europe that idiosyncratic hepatotoxicity associated with use ofherbal medicines may not be identified because the population taking herbal medicines isnot large enough to produce sufficient cases for the association to be noted. But the factthat kava remains in traditional usage to such a wide extent is a powerful argument thatidiosyncratic hepatotoxicity would have been noted.
Two post-marketing observation studies in Germany each on over 3,000 people are cited byPittler & Ernst (2000), in addition to the clinical trials already mentioned above. In theseobservational studies, the rate of adverse events was 2.3% (daily dose of kava lactones120-240mg) and 1.5% (daily dose 105 mg) lactones. The most frequent adverse reportswere gastrointestinal complaints, allergic skin reactions, headache and photosensitivity. There is evidence in the South Pacific of a characteristic kava-induced skin disease which isdescribed as a scaly rash suggestive of icthyosis (Ruze, 1990) - a condition called “kavadermopathy”. Although the skin becomes yellow, the description does not suggest anunderlying hepatic condition in that the patient remains well, the rash is not itchy and thecondition improves without treatment if the heavy use of kava is reduced. Discussion of alleged Kava hepatotoxicity and the cases reported by BfArM Hepatotoxicity
The German and Swiss reports cited by BfArM are of concern because there have beenprevious reports of hepatotoxicity associated with the use of medicinal plants (Larrey,1997). The kava case reports from BfArM include all three of the main forms of acutedamage to the hepatocyte which can result from adverse drug reactions i.e. necrosis, drug -induced hepatitis and cholestatic hepatitis (Hodgson & Levi, 1997). This suggests that thereis a range of causes rather than just one cause in the reported cases. Discussion of the cases reported by BfArM The cases are numbered on the basis of the identifier in the table in English provided by BfArM to the Medicines Control Agency. They are discussed on the basis of our translation of the section describing the cases “Draft statement of two German pharmaceutical associations, Bundersverband der Arzneimittel Herstell e. V. (BAH) and Bunderverband der Pharmazeutischen Indusctrie e. V. ( BPI)” subsequently referred to as BAH. The cases are identical except for case 3 which is not included in the BAH report. The BAH report claims that a number of the cases have been reported in the literature more than once, including case 28, and, in particular that cases 7 and 8 (BAH 5.16) are the same case and that cases 26 and 27 (BAH 5.12) are the same case. The details agree except for case 4 (BAH 5.8) where a different time before onset is given and for cases 23 and 25 (both included as BAH 5.6) where the time before onset of the two cases is reversed.
These discrepancies in numbering are unsatisfactory and tend to undermine confidence inthe accuracy and veracity of the information provided by BfArM.
The BfArM document is deficient in other respects too. The detail it provides is inadequate toevaluate most of the cases cited. In particular, no detail is provided regarding other medicalconditions from which the patients mentioned in the report may have been suffering. Inaddition, the data provided on the eventual outcome of the cases is incomplete. It is alsounclear whether the term “liver damage” refers to the results of a liver biopsy or to thefinding of raised alanine aminotransferase (ALT) blood levels which are interpreted asindicating damage to hepatocytes in hepatocellular disease (Pagana, 1999). However, in thelight of the need for the UK Medicines Control Agency to make an informed decision onthese cases, we have endeavoured to interpret the evidence as presented. Unless notedotherwise, references to possible drug-induced hepatoxocity is taken from the BritishNational Formulary, March 2001. Cases analysed and categorised by common factors of note Case Nos 1,2,19,28 Patients were taking a product made from synthetic kavain. Although, the outcome was hepatitis in all four cases, kavain cannot be equated with the naturally occurring form of kava and therefore no inference should be drawn from these cases. Traditional usage should not be taken as evidence for safe usage of synthetic products. 1. Cases who were taking the oral contraceptive pill or Hormone Replacement Therapytogether with a drug which can also be associated with liver damage Six Cases: Nos 4, 10, 12, 20, 21, 28
Cholestatic jaundice associated with use of oestrogen-containing medications is extremelyrare (Lindberg, 1992) but does occur. In these 6 cases, the woman was also taking a drugwhich can also be associated with jaundice:
Case 4: (BAH 5.8, woman, 39, jaundice) diazepam 10mg PRN for 6 months
Case 10: (BAH 4, woman, 39, necrotizing hepatitis) “several antidepressants includingparoxetine”
Case 12: (BAH 5.15, woman, 37, hepatitis) diclofenac 150mg by intramuscular injection. Hepatotoxic reactions associated with NSAID use are extremely rare and concomitantexposure to other hepatotoxic drugs is considered an important factor (Bareille et al, 2001).
This case is of hepatitis is difficult to interpret as it occurred in Brazil and as “re-exposurewas said to be negative for all three drugs”.
Case 20: (BAH 3, woman, 50, necrosis, liver transplant) this woman had a 20-year historyof combined oral contraceptive use but had changed months earlier to oestradiol valerate(apparently taken alone) as hormone replacement therapy. She had also started glimepride8 months earlier. This is used for type II diabetes and is rarely associated with cholestaticjaundice and liver failure.
Case 21: (BAH 2, woman, 22, necrosis, liver transplant) this woman had changed fromValette (dienogest 2mg and ethinlestradiol 0.03 mg) to Pramino (norgestimate180/215/250mcg and ethinylestradiol 25mcg). She also took rizatriptan if required formigraine relief. Rizatriptan is contra-indicated in hepatic impairment
Case 28 (BAH 5.4, woman, age unknown, hepatitis) this case is hard to interpret as no ageis given and the woman was taking oestradiol valerate “twice weekly”, acetylcysteine,losartan which is rarely associated with hepatitis and omeprazole which can be associatedwith liver disease although, again this is rare (Paseka, 2000). Omeprazole is metabolised bythe polymorphic CYP2C19 which is absent in 3% of Caucasians (Flockhart, 2000). Thewoman was also taking Esberitox (Echinacea) and 5 products which appear to be for upperrespiratory problems - making a total of 11 products. As noted above this patient wastaking synthetic kavain, not kava. 2.Cases who were taking a drug which can be associated with liver damage Ten Cases: Nos 1,6, 9,14, 15, 17, 19,23, 26/27, 29
Case 1: (BAH 5.10, woman, 69, cholestatic hepatitis) was taking pentoxifylline which can beassociated with intrahepatic cholestasis and a diuretic including the potassium-sparingtriamterene which can be associated with jaundice. As noted above this patient was takingsynthetic kavain, not kava.
Case 6: (BAH 5.10, woman, 50, hepatitis) was taking frusemide which can be associatedwith cholestatic jaundice, and triamterene (as above), atenolol, and a large dose ofterfenadine 300mg. The recommended dose in the BNF is 60-120mg and terfenadine shouldalso be avoided in hepatic impairment. The IKS considered this case to be caused byterfenadine.
Case 9: (BAH 5.1, woman, 81, liver failure and subsequent death). She was takinghydrochlorothiazide which can occasionally be associated with intrahepatic cholestasis. However, the autopsy showed chronic pancreatitis, characteristic of alcohol abuse and thereport says that symptoms must have occurred over a period of at least 18 months. Thereport concedes “hepatic impairment by alcohol not excluded”. In these circumstances, itseems entirely reasonable to hold that this case is unrelated to kava use.
Case 14: (BAH 5.11, woman, 33, hepatitis) Cisapride, may have been taken which cancause reversible changes in liver function tests. Cirrhosis in a woman of 33 is anunexplained finding and the detail is inadequate to elucidate this case.
Case 15: (BAH 5.13, woman, 46, jaundice) had been taking hydrochlorothiazide for 5.5months which can be associated with intrahepatic cholestasis and valsartan 80mg andpropanolol 80mg daily.
Case 17: (BAH 5.14, woman, 59, jaundice) Celecoxib, a cyclooxygenase-2 inhibitor, wastaken at 100-200mg daily.
Case 19: (BAH 5.3, woman, 21, hepatitis) was taking pantoprazole which, as withomeprazole, can be associated with liver disease. She was also taking paracetamol andmetoclopramide and had overdosed on Kavain. More detail is needed on other medicalconditions suffered by this patient in order to interpret this case. Further importantinformation regarding this case has come to light as this paper is being submitted and is presented in a footnote.[1]
Case 23: (BAH 5.6 ii, woman, 35, jaundice) paracetamol was also taken but no dosage ordetails are provided.
Case 26/27: (BAH 5.12, woman 38 or 39, hepatitis) The confusion of cases here is anexample of inaccurate data records provided by BfArM. . This case or cases depending onwhether the two reports are of the same woman is unclear. Penicillin can be associated withhypersensitivity and cholestatic jaundice but the information given is inadequate.
Case 29: (BAH 1, woman, 60, liver transplant) this woman of 60 was taking piretamidewhich is a loop diuretic. Frusemide, another loop diuretic, can be associated with cholestaticjaundice. She was also taking a sympatheticomimetic, Etilefrine. The dosage varied but wasup to 480mg (four times the recommended dose).
[1] The young woman in case #19 apparently used a product called "Kavain Harras plus." An
article published late last year by Schmidt (see Journal fur Orthomolecular Medizin 9(4):379-
391; the article is titled: "Lebernebenwirkungen durch Kava-Extrakt") states that this product
is a combination of 30mg synthetic d-l kavain and 250mg of an ethanol extract concentrated
to 8% kavalactones, so delivering an additional 20mg kavalactones. Schmidt also states that
this woman was using up to 10 tablets per day of the product (it seems that the manufacturer
suggest 6 tablets daily) and that there was some discussion, apparently in her medical recordor the BfArM file, that she may also have used Ecstasy (i.e., MDMA - see Brauer et al. 1997.
Liver transplantation for the treatment of fulminant hepatic failure induced by the ingestion of
Source personal correspondence from Michael McGuffin, President, American Herbal Products2. Cases where drugs not associated with liver damage, herbal medicines or dietary supplements or Kavain alone were taken Seven Cases: Nos 2, 7/8, 11, 13, 22, 24, 25
In these cases, detail is limited and no other drug or medication can be implicated. All cases apart from 7/8, where no information is given, are stated to have made a fullrecovery. In some of these cases, it is not clear whether the person was ill or whether liverfunction tests were found to be raised when monitoring.
Case 2: (BAH 5.17, man, 35, cholestatic hepatitis) was taking no other medication
Apart from Cases 18 & 30, this is the only case where no other medicationwas taken. As noted above this patient was taking synthetic kavain, not kava.
(BAH 5.9, woman, 68 or 69, cholestatic hepatitis) was taking Neuroplant forte(Hypericum) which has been associated with induction of CYP3A4. Biopsyshowed “immunological hypersensitivity”.
(BAH 5.16, woman or women, age 72 and/or 75, cholestatic hepatitis) wastaking two herbal/vitamin products one of which included 0.6mg of kavalactones.
(BAH 5.19, woman, 59?) was taking Buscopan
(BAH 5.18, woman, 62, jaundice) there was concomitant medication but nodetails and no detail of Kava dosage which makes interpretation impossible
(BAH 5.20, woman, 34, hepatitis) was taking L-thyroxine
(BAH 24, woman, 47, raised liver function test results) was taking fish oils. The report states that the liver enzymes returned to normal when the fish oils
were stopped but again the detail is insufficient. However, this case wouldappear to support the safe use of kava for the report states that the patientwas “restored to health after discontinuation of the concomitant medicationand continuation of the (kava) medication”.
(BAH 5.6 I, woman, 34, hepatitis) was taking Hypericum perforatum4.Associated with an overdose of alcohol
(BAH 5.21, woman, 33, jaundice) took an overdose of alcohol, 60g. This case
is described in detail by Russman et al (2001) and is discussed below as the womanwas shown to be a poor metaboliser of CYP 2D4. 5.Cases not associated with other drug usage Cases 18, 30
The final two cases are men both of whom required liver transplants and both of whomappear not to have been taking other medication. In these two cases, Kava would appear tobe implicated but again more detail of the medical history is required for a properassessment.
(BAH 5.22, man, 50, necrosis, liver transplant) took Laitan 210-280mg dailyfor 1.5 months, “moderate alcohol” and a yeast preparation. This is aboverecommended dose of kavalactones
(BAH 5.2, man, 32, necrosis, liver transplant) took Antares, 240mg daily for 3months and occasionally Baldrian-phyton (Valerian) at night. This too is abovethe recommended dose of kavalactones. Summary In most of the case reports, the patient was also taking drugs concomitantly. Assuming the medication were responsible for the adverse event, and not some other factor such as other disease or excessive use of alcohol, it is possible that the hepatotoxicity was caused by the conventional drug, by the kava, by both the drug and the kava or mainly by the drug but the kava as a co-factor. However, in assessing these cases, we should take into account the increased risk of adverse effects on the liver where kava lactone concentration is enhanced in a product and glutathione presence is reduced due the extraction techniques employed as explained in the paper by Whitton et al (see Appendix 1). Such stress on the liver is still further likely to be enhanced due to individual variability in the metabolic cytochrome P450 processes that are discussed below. Inter-individual variability in cytochrome-P450 metabolism of xenobiotics Inter-individual variability in drug response is now increasingly recognised as a major cause of adverse drug reactions. Much of this variability is now ascribed to genetic differences in drug absorption, disposition, metabolism or excretion. The variability which has been most investigated and which is considered to be of most significance is genetic polymorphism in drug metabolising enzymes in the hepatocyte. This is considered to be an adaptive response to environmental challenge (Wolf, Smith, 1999) so it is not in itself surprising that individuals vary and failure of metabolism of xenobiotics (“foreign” compounds, whether natural or synthetic) is associated with the use of medicines either from natural or synthetic sources.
Cytochrome P450 (CYP) enzymes are mixed function microsomal monooxygenases locatedon smooth endoplasmic reticulum throughout the body primarily in hepatocytes and the wallof the small intestine. There are 12 families and a single hepatocyte can contain a range ofCYP enzymes which metabolise a range of drugs. They are responsible for Phase I
(oxidation, reduction and hydrolysis) metabolism of a wide number of compounds andtransform lipophilic drugs to more polar compounds that can be excreted by the kidneys. Phase II of detoxification occurs if the product conjugates in the hepatocyte cytoplasm withthe tripeptide glutathione. The resulting soluble compound is excreted via the bile or urine. This conjugation is catalysed by cytoplasmic glutathione S-transferases. Interindividualvariations exist in concentration of hepatocyte glutathione and in relative concentration ofindividual glutathione S-transferases (Mannervik, Widdersten, 1995). and in levels of othercompounds associated with drug metabolism. CYP2D6 Deficiency Many CYP enzymes are genetically polymorphic and thus there is marked inter-individual variation in drug metabolism (Wolf, Smith, 1999). One of the most extensively studied genetic polymorphism is that of CYP2D6 and it is considered to cause much of the individual variation seen in drug response, side effects and drug interactions (Poolsup et al, 2000). Individuals may be poor (slow) metabolisers, intermediate, extensive (fast) or ultra-fast metabolisers. In a Caucasian population 7-9% of individuals are homozygous deficient in CYP2D6 and are thus poor (slow) metabolisers (Poolsup, et al, 2000). The incidence of CYP2D6 deficiency in Asian populations is 1% and it is thought that much ethnic variation in drug response is associated with CYP polymorphism (Poolsup, et al, 2000). Drug substrates for CYP2D6 include: antidepressants, antipsychotics, beta-blockers eg propanolol and anti- arrythmics. CYP2D6 metabolizes a range of antidepressants (Fromm, et al., 1997). Poor metabolisers are at risk of adverse reactions if the rate of biotransformation is inadequate.
If xenobiotics are inadequately metabolised they may make covalent bonds with DNA, RNA,nuclear proteins or cytoplasmic proteins and breakdown of function occurs within thesecells. Above a certain rate, the result of this is damage to the hepatocyte leading tocentrilobular necrosis (Kaplowitz, 1997).
Russmann et al (2001) discuss Case 16 in detail. It is noteworthy that the woman hadrestarted kava for three weeks after an initial course of treatment two months earlier andthen became ill three weeks later after an overdose of alcohol. The woman was shown to beCYP2D6 deficient using phenotyping with debrisoquine. The authors then tested Case 10,described by Strahl et al (1998) and found her to also be CYP2D6 deficient and argue thatCYP2D6 deficiency is a risk factor for hepatotoxicity ascribed to kava.
This finding may help to explain the lack of hepatotoxicity due to Kava recorded in theSouth Pacific. Wanwirolmuk et al (1998, cited in Poolsup et al, 2000) tested the phenotypeof 100 Polynesians using a debrisoquine probe and found a 0% incidence of CYP2D6deficiency.
As stated, many antidepressants are metabolised by CYP2D6 and it is likely that the use ofantidepressants with kava is not uncommon. Yet only one of the above cases involvedantidepressants which suggests that CYP2D6 deficiency is more likely to be relevant thancompetition between CYP2D6 substrates.
This finding is significant but difficult to predict as most people are unaware of their CYP2D6phenotype. It should be noted that where CYP2D6 deficiency occurs, kava products withenhanced kava lactones might have implications for the liver particularly when aconcomitant orthodox medicine or substantial amounts of alcohol are regularly taken. Suchrisks are likely to be small if low-alcohol tinctures are employed within the normaltherapeutic dosage range. Recommendations from TMEC: 1. Products made from synthetic Kavain are synthetic drugs not herbal medicinal products and should be excluded from the analysis.
2. None of the cases cited by BfArM involved traditionally prepared tinctures. In the light of evidence presented above and in Appendix 1, the safety of concentrated standardised products made from acetone extracts and high alcohol concentrations needs re-evaluation. Low-alcohol tinctures appear to provide a safe alternative. TMEC recommends the adoption of extraction methods using 25% alcohol that will ensure the extraction of the full spectrum of constituents and a substantially lower concentration of kava lactones thus ensuring the safe use of kava as a medicine. 3. Consumers need to be informed that Kava products should not be taken whilst taking conventional medicines without the advice of a health professional. Kava should not be taken without consulting a health professional if the user has a history of liver disease. 4. Maximum doses for Kava should be set after consultation with interested parties. 5. Doctors, nurses, pharmacists and other health professionals should be adequately informed about herbal medicines and possible herb/ drug interactions (Jobst et al, 2000). Comment The training of health professionals is outside the scope of the Medicines Control Agency. However, the achievement of statutory self-regulation of herbal practitioners would support the endeavours of the professional associations which form the European Herbal Practitioners Association to assure high standards of training and mandatory continuing professional development for those who regularly prescribe herbal medicines to patients. References Andersson, T., 1006. Pharmacokinetics, metabolsm and interactions of acid pump Inhibitors. Focus on omeprazole, lansoprazole and pantoprazole. Clinical Pharmacokinetics 31(1), 9-28 Anon, 1983. British Herbal Pharmacopeia. Keighley: British Herbal Medicine Association BAH. 2001. Summary translation of section describing the cases in “Draft statement of two German pharmaceutical associations, Bundersverband der Arzneimittel Herstell e. V. (BAH) and Bunderverband der Pharmazeutischen Indusctrie e. V. ( BPI)” summary translation, Angela Grunwald on behalf of TMEC Bareille, M., et al., 2001. Liver damage and NSAID: case non-case study in the French Pharmacovigilance Database. Therapie 56 (1), 51-5 Barnes, J., et al., 2001. St John's wort (Hypericum perforatum L.): a review of its chemistry, pharmacology and clinical properties.Journal of Pharmacy and Pharmacology 53(5), 583- 600 Chanwai, L., 2000. Kava toxicity. Emergency Medicine 12, 142-145 Clough, A., et al. 2000. Kava in Arnhem Land: a review of consumption and its social correlates. Drugs and Alcohol Review 19(3), 319-323 De Leo, V., et al., 2001. Evaluation of combining kava extract with hormone replacement therapy in the treatment of postmenopausal anxiety. Maturitas 39, 185-188 Ellingwood, F. 1919. American Materia Medica, Therapeutics and Pharmacognosy. Reprinted by Oregon: Ec;lectic Medical Publications Felter, H., Lloyd, J. 1903 reprinted 1983. King’s American dispensatory. Portland: Eclectic Medical Publications Flockhart, D., et al. 2000. Selection of drugs to treat gastro-oesophageal reflux disease: the role of drug interactions. Clinical Pharmacokinetics 39(4), 295-309
Fromm, M., et al., 1997. Impact of P450 genetic polymorphism on the first-pass extractionof cardiovascular and neuroactive drugs. Advanced Drug Delivery Reviews 27, 171-199Greenwood-Robinson, M. 1999. Kava. Dell PublishingGrunze H, et al. 2001. Kava pyrones exert effects on neuronal transmission andtransmembraneous cation currents similar to established mood stabilizers--a review. ProgNeuropsychopharmacol Biol Psychiatry 25(8), 1555-70Haberlein, H., et al., 1997. Piper methysticum: enantiomeric separation of kavapyrones byHPLC. Planta Medica 63, 63-65He, X, et al., 1997. Electrospray HPLC-MS in phytochemical analysis of Kava (pipermethysticum ) extract. Planta Medica 63, 70-74Hodgson, E., P.E.Levi, 1997. Textbook of modern toxicology. Connecticut: Appleton & LangeJobst, K. et al. 2000. Safety of St Johns Wort (Hypericum perforatum). Lancet 9203, 575Johnson, T. 1999. CRC ethnobotany desk reference. Florida: CRC PressKaplowitz, N. 1997 Hepatotoxicity of Herbal Remedies: Insights into the intricacies of plant-animal warfare and cell death. Gastroenterology 113 (4), 1408-1412Kircheiner, J., et al., 2001. CYP2D6 and CYP2C19 genotype-based dose recommendationsfor antidepressants. Acta Psychiatrica Scandinavia 104, 173-192Kubatova, A., et al. Comparison of subcritical water and organic solvents for extreactingkava lactones from kava root. Journal of Chromatography A, 923, 187-194Larrey, D. 1997. Hepatotoxicity of herbal remedies. Journal of Hepatology 26 (Suppl. 1, 47-51Lebot, V., et al., 1997. Kava - the Pacific Elixir. Vermont: Healing Arts PressLindberg, M. 1992. Hepatobiliary complications of oral contraceptives. Journal of GeneralInternal Medicine 7(2), 199-209Mannervik, B, Widersten, M. (1995) in ed. Pacifici, G,, Fracchia, G., Advances in DrugMetabolism in Man. Brussels: European CommissionMills, S., Bone, K., 2000. Principles and Practice of Phytotherapy Edinburgh: ChurchillLivingstoneMurray, W. 2000. Neoliberal Gloobalisation, “Exotic” Agro-exports, and local change in theislands: A studdy of the fijian kava sector. Singapore Journal of Tropical Geography 21 (3),355-373Pagana, K., Pagana, T. 1999. Mosby’s Diagnostic and Laboratory Test Reference Missouri:MosbyPaseka, 2000Pittler, M., Ernst, E., 2000. Efficacy of Kava Extract for Treating Anxiety: Systematic Reviewand Meta-Analysis. Journal of Clinical Psychopharmacology 20(1), 84-89Poolsup, N., et al., 2000. Pharmacogenetics and phychopharmacotherapy. Journal of ClinicalPharmacy and Therapeutics 25, 197-220Russmann, S., et al., 2001. Kava hepatotoxicity. Annals of Internal Medicine, 135(1), 68-69. Ruze, P., 1990. Kava-induced dermopathy: a niacin deficiency? The Lancet 335, 1442-1445Schulz, V., et al. 1997. Rational phytotherapy. Heidelberg: Springer-VerlagSpinella, M. 2001. The Psychopharmacology of Herbal Medicine. Massachusetts: MIT PressWhitton, P., et al. 2002. Awaiting publication See Appendix 1. Williamson, E.2001. Synergy and other interactions in phytomedicines Phytomedicine 8(5),401-409Wolf, C., Smith, S. 1999. Pharmacogenetics. British Medical Bulletin, 55(2), 366-386
APPENDIX 1. To submission of Traditional Medicines Evaluation Committee (a subcommitteeof the European Herbal Practitioners Association). Response to Reported Hepato-toxicity of High Lactone Extractions of Piper methysticum Forst. (Kava)
P.Whitton PhD student, University of Westminster Dept of Biosciences.
Dr. J.Whitehouse PhD. Senior Lecturer in Herbal Medicine University of Westminster.
Prof. C.Evans BSc. PhD. Head of School of Biosciences, University of Westminster. Introduction This paper (the result of work currently in progress) is produced in response to the reports by the German BfArM of possible hepatotoxic effects of kava extracts that has lead to concerns regarding the safety of kava products on sale in the United Kingdom. There have been thirty cases of hepatotoxicity reported to German and Swiss regulators including three transplants and one death allegedly associated with the use of concentrated standardised kava extracts.
In the Oceanic Islands of the South Pacific kava is drunk as an alternative to alcohol or forceremonial purposes and studies have shown that in islanders who regularly drink up to tentimes the recommended therapeutic dose, the only recorded abnormality is a slightly raisedgamma-glutamyltransferase (Barguil, 2001).
Analysis presented in this paper, based on as yet unpublished research by the authors,demonstrates the presence of glutathione in the traditional extract, which, it is postulated,may have a hepato-protective effect. Concentrated standardised extracts do not containglutathione (see below). Extraction Techniques In the Oceanic Islands, kava is traditionally prepared by macerating the root or root bark in a cold water and/or coconut milk solution. However, in the manufacture of concentrated extracts either ethanol (60% and above) or acetone (60% or above) are employed as solvents to obtain the maximum yield of kava lactones (source Lamberts Ltd) that have been identified as the “active constituent”. Research Data (The result of as yet unpublished work in progress) Analysis of Kava Extraction in Different Solvents Kava (Piper methysticum) root was extracted in different solvents and analysed by High Performance Liquid Chromatography (HPLC) with diode array detection. Different solvents were used to extract the kava lactones, and their extraction is shown in Table 1 below. Table 1:Extraction of kava lactones in different solvents, summary of results for ten samples in each solvent.
The extraction was carried out by reflux percolation for one hour for each sample of 5% w/vPiper methysticum root. The resulting liquids then had their specific gravity and percentagedry extract determined by the techniques described in the British Pharmacopoeia, 1999. Thetotal kava lactones were measured by HPLC using an acetonitrile/ water solvent gradient(Whitton 2001). Kava lactone standardised extracts are produced using a high acetone or ethanolconcentration, and are likely to contain only kava lactones and no proteins, amino acids orsugars.
Further analysis identified one of the other compounds in the aqueous extract and in the25% ethanol extract as glutathione by comparison with a reference sample obtained fromSigma-Aldrich (Poole).
Samples of commercially available kava extracts were examined and the ratio of kava lactones to glutathione was calculated, the results are shown below in Table 2. Table 2: Kava lactone /Glutathione ratios (results summarised from ten samples of each type)
Kava lactone content Glutathione content Kava lactone /(expressed as
extract powder(30% kavalactones) dissolvedin 25% ethanol82% ethanol
extraction (1 partplant to 3 partssolvent)25% ethanol
extraction (1 partplant to 1 partsolvent)
Fig 1Kava lactone & Glutathione extraction (expressed as a percentage of dry extract) against ethanol percentage in solvent Importance of Glutathione in Kava Extracts Lactones may be hepatotoxic, if not mediated by glutathione and are usually metabolised in the liver by enzymes called lactone hydrolases (Schmidt et al. 1999). It is likely that the high concentration of lactones introduced by concentrated standardised extracts has the potential to saturate the enzymatic detoxification pathways resulting in hepatotoxicity. Glutathione has an essential role in the phase II conversion of lactones into excretable waste products. Increased toxicity of the lactones may occur on glutathione depletion. Glutathione is not soluble in ethanol concentrations above 50% (Merck Index). There has been relevant work on a related group of compounds, sesquiterpene lactones. It has been demonstrated that sesquiterpene lactones react with the sulphide group on the glutathione molecule in a reversible pH dependent reaction (Schmidt et al. 1999). The binding of the sesquiterpenes lactones to the glutathione molecule allows for faster clearance by the lactone hydrolases present in the hepatocytes (Schmidt et al. 2001). It has been demonstrated that glutathione prevents toxicity from other sesquiterpene lactones if
administered at the same time (Lautermann et al). It has also been documented thatglutathione has to be present at the time of ingestion of the kava in order to potentiate themetabolism of the lactones.
Glutathione is present in adequate amounts in most cells in the body but some individualscan have a deficiency linked with cytochrome P450 (Lomaestro BM, Malone M, 1995). Inthese cases, high doses of lactones will lead to rapid depletion in glutathione levels andresult in free lactone exposure in the hepatocytes and consequent tissue damage (Zheng etal). Glutathione supplementation has been shown to correct the deficiency (Kidd, 1997). Itis suggested that the glutathione molecule may not be absorbed intact but may be brokendown into its constituent amino acids and regenerated within the hepatocyte. It has beendemonstrated that glutathione prevents toxicity from other sesquiterpene lactones ifadministered at the same time (Lautermann et al). Summary Hepatotoxic lactones are normally metabolised by lactone hydrolases, which are enhanced by the presence of glutathione. Glutathione naturally occurs in kava, (Piper methysticum Forst.) in a 1:1 ratio with kava lactones and is likely to reduce the likelihood of potential lactone toxicity. In contrast to the traditional crude extract, standardised extracts contain no glutathione whilst containing up to 30 times the kava lactone concentration. It appears that the high kava lactone in standardised extracts depletes the reserves of glutathione in the hepatocytes which could result in liver damage. It would therefore seem prudent to limit the organic solvent level in the extraction of kava to 25% ethanol in order to ensure the preservation of the hepato-protective effect of the glutathione. Tinctures made with 25% ethanol would appear to be safe as a result of this synergistic effect of the glutathione and kava lactones. Conclusions Traditional preparations have had many years of safe usage (Tyler, 1995) and toxicity has only been reported in Europe with concentrated standardised extracts (Escher, 2000). This paper argues that there are significant differences between concentrated extracts and those produced by traditional methods that maintain a satisfactory ratio between glutathione and kava lactones. In traditional extracts, ratios of at least 1:1 kava lactone: glutathione should provide a safe product with hepato-protective action. It would appear that glutathione has an important synergistic action in protecting the liver from potential lactone toxicity. This study suggests that standardised herbal extracts which do not contain all components of the traditional plant extract may have a potential to induce hepatotoxicity in susceptible people (e.g. those taking concomitant orthodox medicines). It is proposed that tinctures manufactured using a traditional cold- maceration process (in 25% ethanol and 75% water) that more nearly approximate to traditional water or coconut milk extracts, or raw plant material are safe in normal subjects. References Barguil, Rapid responses, eBMJ, 21 March 2001 Schmidt et al., Bioorganic and Medicinal Chemistry Volume 7, Issue 9, December 1999, 2849-2855 Merck Index Monograph 4483,Twelfth Edition Lomaestro B M, Malone M, Glutathione in health and disease: pharmacotherapeutic issues. Annals Pharmacother, 1995 ;29:1263-1273 Bioorganic and Medicinal Chemistry, Volume 9, No 8, August 2001, 2189-2194 Kidd M D, Alternative Medicine Review, Volume 2, No 6, 1997 Tyler V E, Tyler’s Honest Herbal. 1995
Escher M, Desmeules J. BMJ, November 2000Whitton PA. Rapid Responses eBMJ, March 2001Zheng, J; Wurz, G T; Cadman, T B; Degregorio, M W; Jones, A D; Hammock,BD. Medlineabstract. Lautermann, J; McLaren, J; Schacht, J Hearing Research,Volume 86, Issue 1-2June 1995, Pages 15-24
Cannabis et Trouble Déficit de l’Attention (TDA) David Bearman, M.D., Californie (USA) http://davidbearmanmd.com/ Traduction autorisée par l’auteur http://mcforadhd.free.fr/ Les symptômes principaux des types les plus connus du TDAH (Trouble Déficit de l’Attention / Hyperactivité) sont (1) suractivité motrice, (2) inattention et (3) impulsivité (American Psychiatric Associat
BETEGTÁJÉKOZTATÓ A BASEDOW-KÓR OKOZTA PAJZSMIRIGY-TÚLMÛ KÖDÉSRÕ L Az esetek nagy részében igen kellemetlen tünetekkel járó betegségrõl van szó. Szerencsére abetegség gyakorlatilag mindenkinél nagyon jól gyógyítható. A kezdeti nagyon kellemetlentüneteket kivétel nélkül hatékonyan meg lehet szüntetni. A betegség igazi problémáját kétdolog jelenti: az egyik

 Response to concerns about Piper methysticum Forst. f., Kava. A
Response to concerns about Piper methysticum Forst. f., Kava. A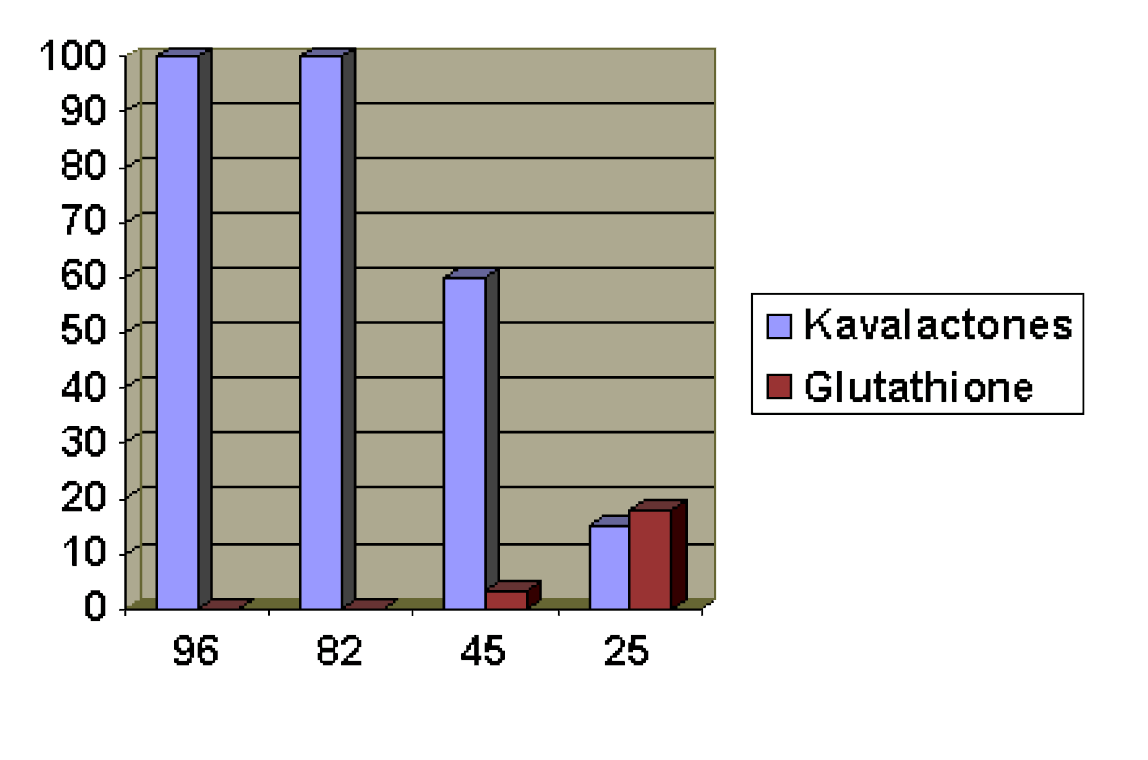 Table 2: Kava lactone /Glutathione ratios (results summarised from ten
Table 2: Kava lactone /Glutathione ratios (results summarised from ten